Journal of Peking University(Health Sciences) ›› 2020, Vol. 52 ›› Issue (1): 152-157. doi: 10.19723/j.issn.1671-167X.2020.01.024
Previous Articles Next Articles
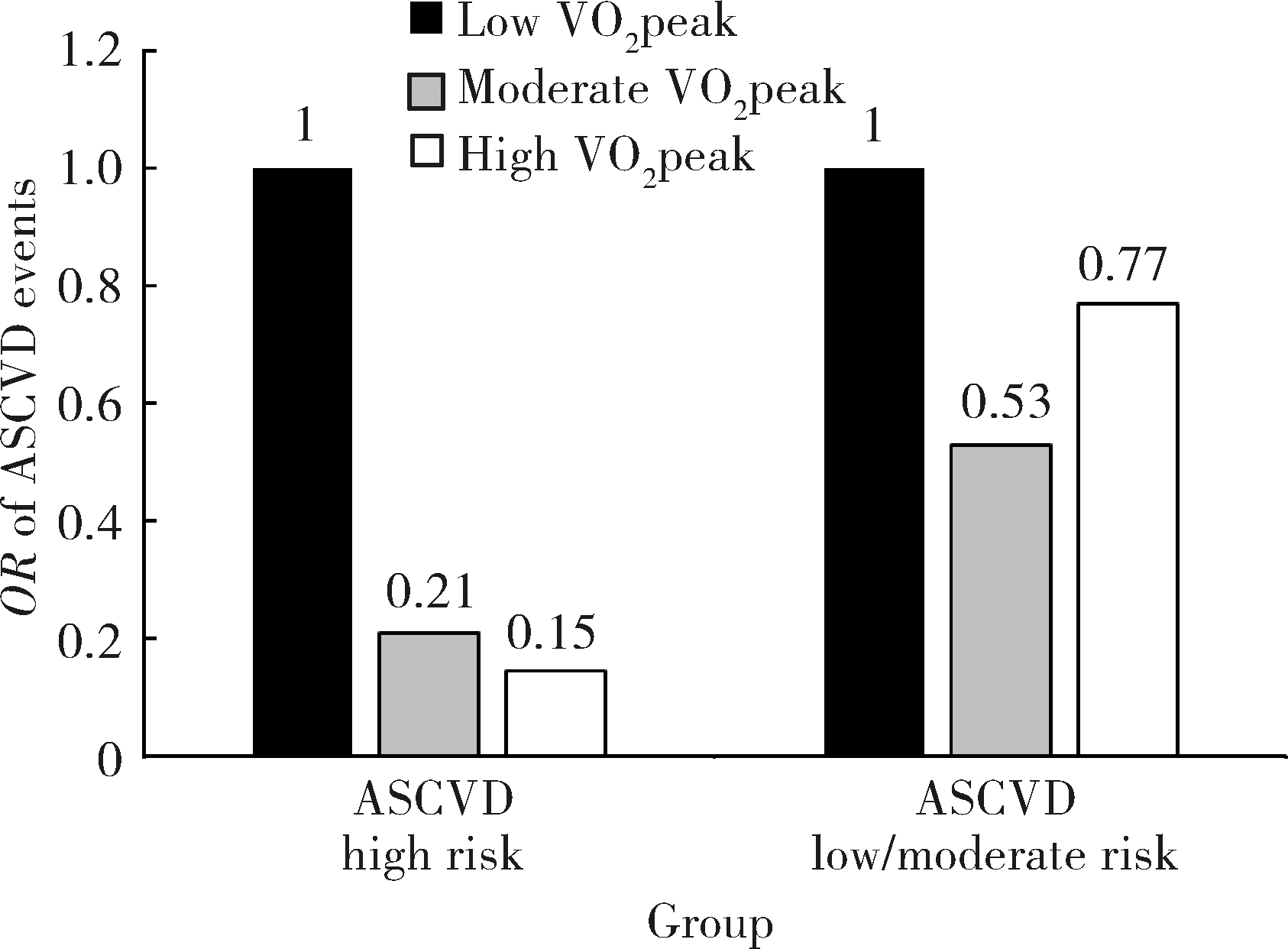
Protective effect of cardiopulmonary fitness on patients with high risk of atherosclerotic cardiovascular disease
Chuan REN1,Xiao-yue WU1,Wei ZHAO1,2,△( ),Li-yuan TAO3,Ping LIU1,Wei GAO1
),Li-yuan TAO3,Ping LIU1,Wei GAO1
- 1. Department of Cardiology, Peking University Third Hospital; Institute of Vascular Medicine of Peking University Third Hospital; Key Laboratory of Cardiovascular Molecular Biology and Regulatory Peptides of National Health Commission; Key Laboratory of Molecular Cardiovascular Science of Ministry of Education; Beijing Key Laboratory of Cardiovascular Receptors Research, Beijing 100191, China
2. Physical Examination Center, Peking University Third Hospital, Beijing 100191, China
3. Research Center of Clinical Epidemiology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R541.4

| [1] | Ross R, Blair SN, Arena R , et al. Importance of assessing cardiorespiratory fitness in clinical practice: A case for fitness as a clinical vital sign: A scientific statement from the American Heart Association[J]. Circulation, 2016,134(24):e653-e699. |
| [2] | Hannan AL, Hing W, Simas V , et al. High-intensity interval training versus moderate-intensity continuous training within cardiac rehabilitation: A systematic review and meta-analysis[J]. Open Access J Sports Med, 2018,9:1-17. |
| [3] | Letnes JM, Dalen H, Vesterbekkmo EK , et al. Peak oxygen uptake and incident coronary heart disease in a healthy population: the HUNT fitness study[J]. Eur Heart J, 2019,40(20):1633-1639. |
| [4] | 中国成人血脂异常防治指南修订联合委员会. 中国成人血脂异常防治指南(2016年修订版)[J]. 中国循环杂志, 2016,31(10):937-951. |
| [5] | Skalski J, Allison TG, Miller TD , et al. The safety of cardiopulmonary exercise testing in a population with high-risk cardiovascular diseases[J]. Circulation, 2012,126(21):2465-2472. |
| [6] | Stamatakis E, Hamer M, O'Donovan G , et al. A non-exercise testing method for estimating cardiorespiratory fitness: Associations with all-cause and cardiovascular mortality in a pooled analysis of eight population-based cohorts[J]. Eur Heart J, 2013,34(10):750-758. |
| [7] | Gander J, Lee DC, Sui X , et al. Self-rated health status and cardiorespiratory fitness as predictors of mortality in men[J]. Br J Sports Med, 2011,45(14):1095-1100. |
| [8] | Kim D, Park W . The inverse relationship between cardiorespiratory fitness and intima- media thickness with prehypertensive middle-aged woman[J]. Tohoku J Exp Med, 2017,243(4):283-288. |
| [9] | Brawner CA, Al-Mallah MH, Ehrman JK , et al. Change in maximal exercise capacity is associated with survival in men and women[J]. Mayo Clin Proc, 2017,92(3):383-390. |
| [10] | Ehrman JK, Brawner CA, Al-Mallah MH , et al. Cardiorespiratory fitness change and mortality risk among black and white patients: Henry Ford Exercise Testing (FIT) project[J]. Am J Med, 2017,130(10):1177-1183. |
| [11] | Kelley E, Imboden MT, Harber MP , et al. Cardiorespiratory fitness is inversely associated with clustering of metabolic syndrome risk factors: The ball state adult fitness program longitudinal life-style study[J]. Mayo Clin Proc Innov Qual Outcomes, 2018,2(2):155-164. |
| [12] | Mora S, Redberg RF, Cui Y , et al. Ability of exercise testing to predict cardiovascular and all-cause death in asymptomatic women: A 20-year follow-up of the lipid research clinics prevalence study[J]. JAMA, 2003,290(12):1600-1607. |
| [13] | Barker AR, Gracia-Marco L, Ruiz JR , et al. Physical activity, sedentary time, TV viewing, physical fitness and cardiovascular disease risk in adolescents: The HELENA study[J]. Int J Car-diol, 2018,254:303-309. |
| [14] | Williams PT . Physical fitness and activity as separate heart disease risk factors: A meta-analysis[J]. Med Sci Sports Exerc, 2001,33(5):754-761. |
| [15] | Ekblom-Bak E, Hellénius ML, Ekblom O , et al. Independent associations of physical activity and cardiovascular fitness with cardiovascular risk in adults[J]. Eur J Cardiovasc Prev Rehabil, 2010,17(2):175-180. |
| [16] | Pinkstaff S, Peberdy MA, Kontos MC , et al. Overestimation of aerobic capacity with the bruce treadmill protocol in patients being assessed for suspected myocardial ischemia[J]. J Cardiopulm Rehabil Prev, 2011,31(4):254-260. |
| [1] | Qi MIAO, Baoan HONG, Xuezhou ZHANG, Zhipeng SUN, Wei WANG, Yuxuan WANG, Yuxuan BO, Jiahui ZHAO, Ning ZHANG. Risk assessment of perioperative adverse events and management of antiplatelet therapy in patients with bladder cancer and coronary atherosclerotic heart disease undergoing transurethral resection of bladder cancer [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 698-703. |
| [2] | Huan LIU,Ying-dong HE,Jin-bo LIU,Wei HUANG,Na ZHAO,Hong-wei ZHAO,Xiao-hua ZHOU,Hong-yu WANG. Predictive value of vascular health indicators on newly cardiovascular events: Preliminary validation of Beijing vascular health stratification system [J]. Journal of Peking University (Health Sciences), 2020, 52(3): 514-520. |
| [3] | Wen-qiang SUN,Zhou ZHAO,Qing GAO,Zeng-qiang HAN,Wei YANG,Bo LIAN,Gang LIU,Sheng-long CHEN,Yu CHEN. Effects of intraoperative graft flow measurements on the early mid-term outcomes after off-pump coronary artery bypass grafting [J]. Journal of Peking University(Health Sciences), 2019, 51(5): 851-855. |
| [4] | Jing ZHANG,Su-fang LI,Hong CHEN,Jun-xian SONG. Role of miR-106b-5p in the regulation of gene profiles in endothelial cells [J]. Journal of Peking University(Health Sciences), 2019, 51(2): 221-227. |
| [5] | LIU Teng-fei, ZHANG Jing-wei, CHEN Xia-huan, FENG Xue-ru, BAI Zhong-sheng, LIU Mei-lin. Association between CMTM5 gene rs723840 single nucleotide polymorphism and high on asprin platelet reactivity [J]. Journal of Peking University(Health Sciences), 2015, 47(6): 905-909. |
| [6] | LIU Teng-fei, ZHANG Jing-wei, CHEN Xia-huan, FENG Xue-ru, BAI Zhong-sheng, LIU Mei-lin. Correlation between the level of the urinary 11-dehydrothromboxane B2 and the clinical efficacy of aspirin in patients with type 2 diabete and coronary artery disease [J]. Journal of Peking University(Health Sciences), 2015, 47(6): 920-924. |
|
||