Journal of Peking University (Health Sciences) ›› 2020, Vol. 52 ›› Issue (2): 234-239. doi: 10.19723/j.issn.1671-167X.2020.02.007
Previous Articles Next Articles
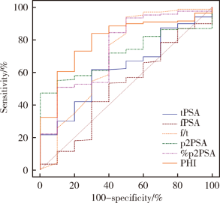
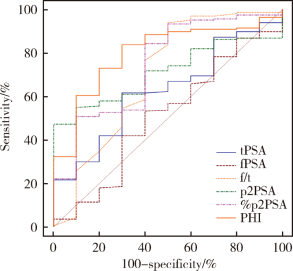
Clinical value of serum isoform [-2] proprostate-specific antigen and its derivatives in predicting aggressive prostate cancer
Kui-xia SUN,Cun-ling YAN( ),Zhi-yan LI,Ping LIU,Wei ZHANG,Qun HE
),Zhi-yan LI,Ping LIU,Wei ZHANG,Qun HE
- Department of Clinical Laboratory, Peking University First Hospital, Beijing 100034, China
CLC Number:
- R737.2
| [1] | Stephan C, Vincendeau S, Houlgatte A , et al. Multicenter evaluation of [-2]proprostate-specific antigen and the prostate health index for detecting prostate cancer[J]. Clin Chem, 2013,59(1):306-314. |
| [2] | 黄宜, 王文涓, 许静 , 等. p2PSA及其相关指标 PHI 在前列腺癌诊断中的应用价值[J]. 检验医学, 2019,34(7):600-604. |
| [3] | Quinn D, Gross M . Show us a sign: the search for "game changing" prostate cancer biomarkers[J]. Lancet Oncol, 2011,12(3):204-206. |
| [4] | Vukovic I, Djordjevic D, Bojanic N , et al. Predictive value of [-2]propsa(p2psa) and its derivatives for the prostate cancer detection in the 2.0 to 10.0 ng/mL PSA range[J]. Int Braz J Urol, 2017,43(1):48-56. |
| [5] | 朱耀, 唐钵, 戴波 , 等. 前列腺健康指数在中国男性前列腺癌诊断中的应用研究[J]. 中华外科杂志, 2017,55(10):734-737. |
| [6] | 闫存玲, 李志艳, 何群 , 等. 血清前列腺特异性抗原同源异构体-2在前列腺癌中的应用价值[J]. 中华检验医学杂志, 2015,38(12):813-817. |
| [7] | Catalona WJ, Partin AW, Sanda MG , et al. A multicenter study of [-2]pro-prostate specific antigen combined with prostate speci-fic antigen and free prostate specific antigen for prostate cancer detection in the 2.0 to 10.0 ng/ml prostate specific antigen range[J]. J Urol, 2011,185(5):1650-1655. |
| [8] | Jansen FH, van Schaik RHN, Kurstjens J , et al. Prostate-specific antigen (PSA) isoform p2PSA in combination with total PSA and free PSA improves diagnostic accuracy in prostate cancer detection[J]. Eur Urol, 2010,57(6):921-927 |
| [9] | Fossati N, Buffi NM, Haese A , et al. Preoperative prostate speci-fic antigen isoform p2PSA and its derivatives, %p2PSA and prostate health index, predict pathologic outcomes in patients undergoing radical prostatectomy for prostate cancer: results from a multicentric European prospective study[J]. Eur Urol, 2015,68(1):132-138 |
| [10] | Eminaga O, Bögemann M, Breil B , et al. Preoperative prostate-specific antigen isoform p2PSA ≤ 22.5 pg/ml predicts advanced prostate cancer in patients undergoing radical prostatectomy[J]. Urol Oncol, 2014,32(8):1117-1126. |
| [11] | Guazzoni G, Lazzeri M, Nava L , et al. Preoperative prostate-specific antigen isoform p2PSA and its derivatives, %p2PSA and prostate health index, predict pathologic outcomes in patients undergoing radicalprostatectomy for prostate cancer[J]. Eur Urol, 2012,61(3):455-466. |
| [12] | Schwen ZR, Tosoian JJ, Sokoll LJ , et al. Prostate Health Index (PHI) Predicts High-stage Pathology in African American Men[J]. Urology, 2016,90:136-140. |
| [13] | Dolejsova O, Kucera R, Fuchsova R , et al. The ability of Prostate Health Index (PHI) to predict gleason score in patients with prostate cancer and discriminate patients between gleason score 6 and gleason score higher than 6: a study on 320 patients after radical prostatectomy[J]. Technol Cancer Res Treat, 2018,17:1-6. |
| [14] | Chiu PK, Lai FM, Teoh JY , et al. Prostate health index and %p2PSA predict aggressive prostate cancer pathology in Chinese[J]. Ann Surg Onclo, 2016,23(8):2707-2714. |
| [15] | 王友林, 朱磊一, 姜波 , 等. 超声引导下经直肠前列腺穿刺与前列腺癌根治术后病理组织Gleason评分差异性的研究[J]. 临床泌尿外科杂志, 2015,30(7):628-630. |
| [1] | Jie LIU, Mingwei MA, Qing'an WANG, Ming SHI, Jinpeng YIN, Zhanping WANG, Jingtao SHEN, Xianshu GAO. Comparison of setup errors between two immobilization methods in prostate cancer radiotherapy based on cone-beam computed tomography [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 692-697. |
| [2] | Ye YAN,Xiaolong LI,Haizhui XIA,Xuehua ZHU,Yuting ZHANG,Fan ZHANG,Ke LIU,Cheng LIU,Lulin MA. Analysis of risk factors for long-term overactive bladder after radical prostatectomy [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 589-593. |
| [3] | Sheng-jie LIU,Hui-min HOU,Zheng-tong LV,Xin DING,Lu WANG,Lei ZHANG,Ming LIU. Bipolar androgen therapy followed by immune checkpoint inhibitors in metastatic castration resistant prostate cancer: A report of 4 cases [J]. Journal of Peking University (Health Sciences), 2022, 54(4): 766-769. |
| [4] | BAI Gao-chen,SONG Yi,JIN Jie,YU Wei,HE Zhi-song. Clinical efficacy of docetaxel combined with carboplatin in patients with metastatic castration-resistant prostate cancer [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 686-691. |
| [5] | Wen-qing LI,Si-mei REN,Xing-bo LONG,Yu-qing TIAN. Palmitoylome profiling indicates that androgens promote the palmitoylation of metabolism-related proteins in prostate cancer-derived LNCaP cells [J]. Journal of Peking University (Health Sciences), 2020, 52(2): 227-233. |
| [6] | Kuan-gen ZHANG,Yu-he ZHOU,Ya-kun SHAO,Fang MEI,Jiang-feng YOU,Bei-ying LIU,Fei PEI. Novel tumor metastasis suppressorgene LASS2/TMSG1 S248A mutant promotes invasion of prostate cancer cells through increasing ATP6V0C expression [J]. Journal of Peking University(Health Sciences), 2019, 51(2): 210-220. |
| [7] | TANG Xu, ZHAO Wei-hong, SONG Qin-qin, YIN Hua-qi, DU Yi-qing, SHENG Zheng-zuo, WANG Qiang, ZHANG Xiao-wei, LI Qing, LIU Shi-jun, XU Tao. Influence of SOX10 on the proliferation and invasion of prostate cancer cells [J]. Journal of Peking University(Health Sciences), 2018, 50(4): 602-606. |
| [8] | ZOU Peng-cheng, YANG Yi-feng, XU Xiao-yan LIU Bei-ying, MEI Fang, YOU Jiang-feng, LIU Qi-chen, PEI Fei . Silencing of vacuolar ATPase c subunit ATP6V0C inhibits invasion of prostate cancer cells [J]. Journal of Peking University(Health Sciences), 2017, 49(6): 937-947. |
| [9] | JI Guang-jie, HUANG Cong, SONG Gang, LI Xue-song, SONG Yi, ZHOU Li-qun. Predictive factor analysis of time to progression of castration-resistant prostate cancer after androgen deprivation therapy [J]. Journal of Peking University(Health Sciences), 2017, 49(4): 657-662. |
|
||