Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (4): 728-733. doi: 10.19723/j.issn.1671-167X.2021.04.018
Previous Articles Next Articles
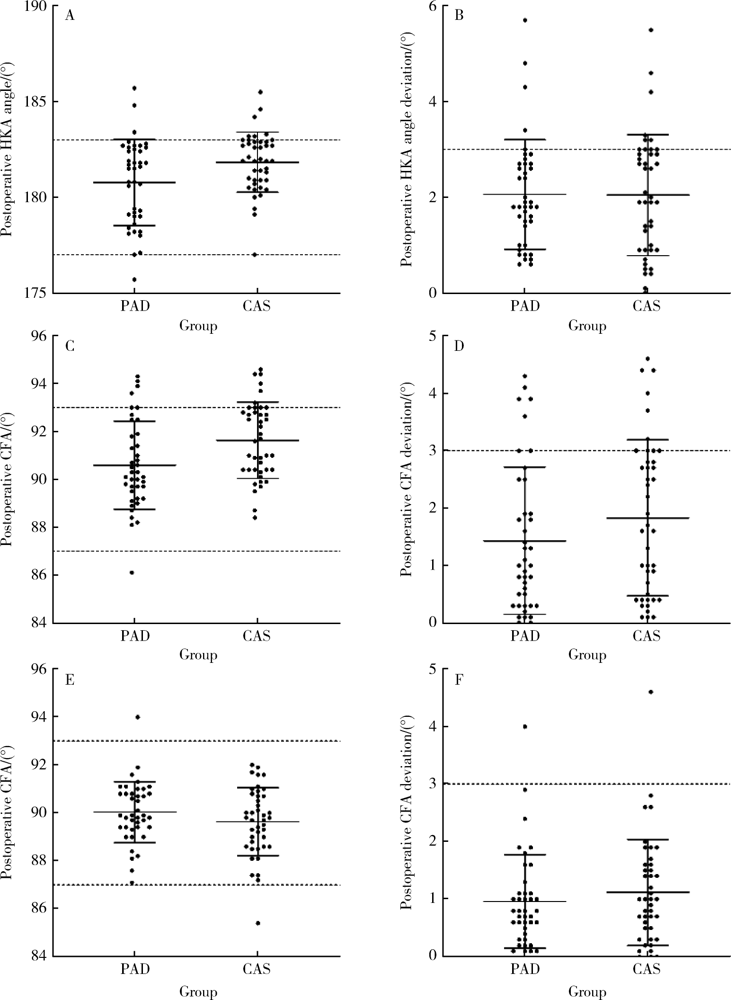
Comparison of alignment and operative time between portable accelerometer-based navigation device and computer assisted surgery in total knee arthroplasty
WANG Xin-guang1,2,GENG Xiao1,2,LI Yang1,2,WU Tian-chen3,LI Zi-jian1,2,Δ( ),TIAN Hua1,2
),TIAN Hua1,2
- 1. Department of Orthopaedics, Peking University Third Hospital, Beijing 100191, China
2. Engineering Research Center of Bone and Joint Precision Medicine, Ministry of Education, Beijing 100191, China
3. Department of Maternal and Child Health, School of Public Health, Peking University, Beijing 100191, China
CLC Number:
- R687.4



| [1] |
Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030 [J]. J Bone Joint Surg Am, 2007, 89(4):780-785.
doi: 10.2106/00004623-200704000-00012 |
| [2] |
Longstaff LM, Sloan K, Stamp N, et al. Good alignment after total knee arthroplasty leads to faster rehabilitation and better function [J]. J Arthroplasty, 2009, 24(4):570-578.
doi: 10.1016/j.arth.2008.03.002 pmid: 18534396 |
| [3] |
Gromov K, Korchi M, Thomsen MG, et al. What is the optimal alignment of the tibial and femoral components in knee arthroplasty [J]. Acta Orthop, 2014, 85(5):480-487.
doi: 10.3109/17453674.2014.940573 |
| [4] | Zhao MW, Wang L, Zeng L, et al. Effect of femoral resection on coronal overall alignment after conventional total knee arthroplasty [J]. Chin Med J (Engl), 2016, 129(21):2535-2539. |
| [5] | 王康, 石一璠, 赵昱, 等. 计算机导航与传统人工全膝关节置换临床疗效的Meta分析 [J]. 中华关节外科杂志:电子版, 2018, 12(2):222-230. |
| [6] |
Sun H, Li S, Wang K, et al. Efficacy of portable accelerometer-based navigation devices versus conventional guides in total knee arthroplasty: a meta-analysis [J]. J Knee Surg, 2020, 33(7):691-703.
doi: 10.1055/s-0039-1685145 |
| [7] | Johnston H, Abdelgaied A, Pandit H, et al. The effect of surgical alignment and soft tissue conditions on the kinematics and wear of a fixed bearing total knee replacement [J/OL]. J Mech Behav Biomed Mater, 2019, 100: 103386 [2020-06-01]. https://www.sciencedirect.com/science/article/pii/S1751616119303388?via%3Dihub . |
| [8] |
Parratte S, Pagnano MW, Trousdale RT, et al. Effect of post-operative mechanical axis alignment on the fifteen-year survival of modern, cemented total knee replacements [J]. J Bone Joint Surg Am, 2010, 92(12):2143-2149.
doi: 10.2106/JBJS.I.01398 |
| [9] |
Rhee SJ, Kim HJ, Lee CR, et al. A comparison of long-term outcomes of computer-navigated and conventional total knee arthroplasty: a meta-analysis of randomized controlled trials [J]. J Bone Joint Surg Am, 2019, 101(20):1875-1885.
doi: 10.2106/JBJS.19.00257 |
| [10] |
Kinney MC, Cidambi KR, Severns DL, et al. Comparison of the iassist handheld guidance system to conventional instruments for mechanical axis restoration in total knee arthroplasty [J]. J Arthroplasty, 2018, 33(1):61-66.
doi: 10.1016/j.arth.2017.06.004 |
| [11] |
Li JT, Gao X, Li X. Comparison of iassist navigation system with conventional techniques in total knee arthroplasty: a systematic review and meta-analysis of radiographic and clinical outcomes [J]. Orthop Surg, 2019, 11(6):985-993.
doi: 10.1111/os.v11.6 |
| [12] |
Desseaux A, Graf P, Dubrana F, et al. Radiographic outcomes in the coronal plane with iassist (tm) versus optical navigation for total knee arthroplasty: a preliminary case-control study [J]. Orthop Traumatol Surg Res, 2016, 102(3):363-368.
doi: 10.1016/j.otsr.2016.01.018 |
| [13] |
Goh GS, Liow MHL, Lim WS, et al. Accelerometer-based navigation is as accurate as optical computer navigation in restoring the joint line and mechanical axis after total knee arthroplasty a prospective matched study [J]. J Arthroplasty, 2016, 31(1):92-97.
doi: 10.1016/j.arth.2015.06.048 |
| [14] |
Goh GS, Liow MHL, Tay DK, et al. Accelerometer-based and computer-assisted navigation in total knee arthroplasty: a reduction in mechanical axis outliers does not lead to improvement in functional outcomes or quality of life when compared to conventional total knee arthroplasty [J]. J Arthroplasty, 2018, 33(2):379-385.
doi: 10.1016/j.arth.2017.09.005 |
| [15] |
Cip J, Obwegeser F, Benesch T, et al. Twelve-year follow-up of navigated computer-assisted versus conventional total knee arthroplasty: a prospective randomized comparative trial [J]. J Arthroplasty, 2018, 33(5):1404-1411.
doi: 10.1016/j.arth.2017.12.012 |
| [16] | Mullaji AB, Shetty GM. Efficacy of a novel ipod-based navigation system compared to traditional navigation system in total knee arthroplasty [J]. Comput Assist Surg (Abingdon), 2017, 22(1):10-13. |
| [1] | WANG Jun-feng, LI Zhao, ZHANG Ke-shi, YUAN Feng, LI Ru-jun, ZHONG Qun-jie, GUAN Zhen-peng. Unilateral patellar resurfacing in bilateral total knee arthroplasty: a randomized controlled study [J]. Journal of Peking University(Health Sciences), 2017, 49(5): 861-866. |
| [2] | ZHAO Min-wei, WANG Ning, ZENG Lin, LI Min, ZHAO Zhong-kai, ZHANG Han, TIAN Hua . Comparision for clinical efficiency of continuous adductor canal block and femoral nerve block in total knee arthroplasty [J]. Journal of Peking University(Health Sciences), 2017, 49(1): 142-147. |
|
||