Journal of Peking University (Health Sciences) ›› 2024, Vol. 56 ›› Issue (4): 594-599. doi: 10.19723/j.issn.1671-167X.2024.04.008
Previous Articles Next Articles
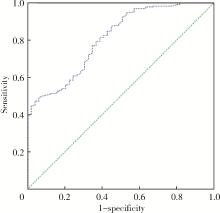
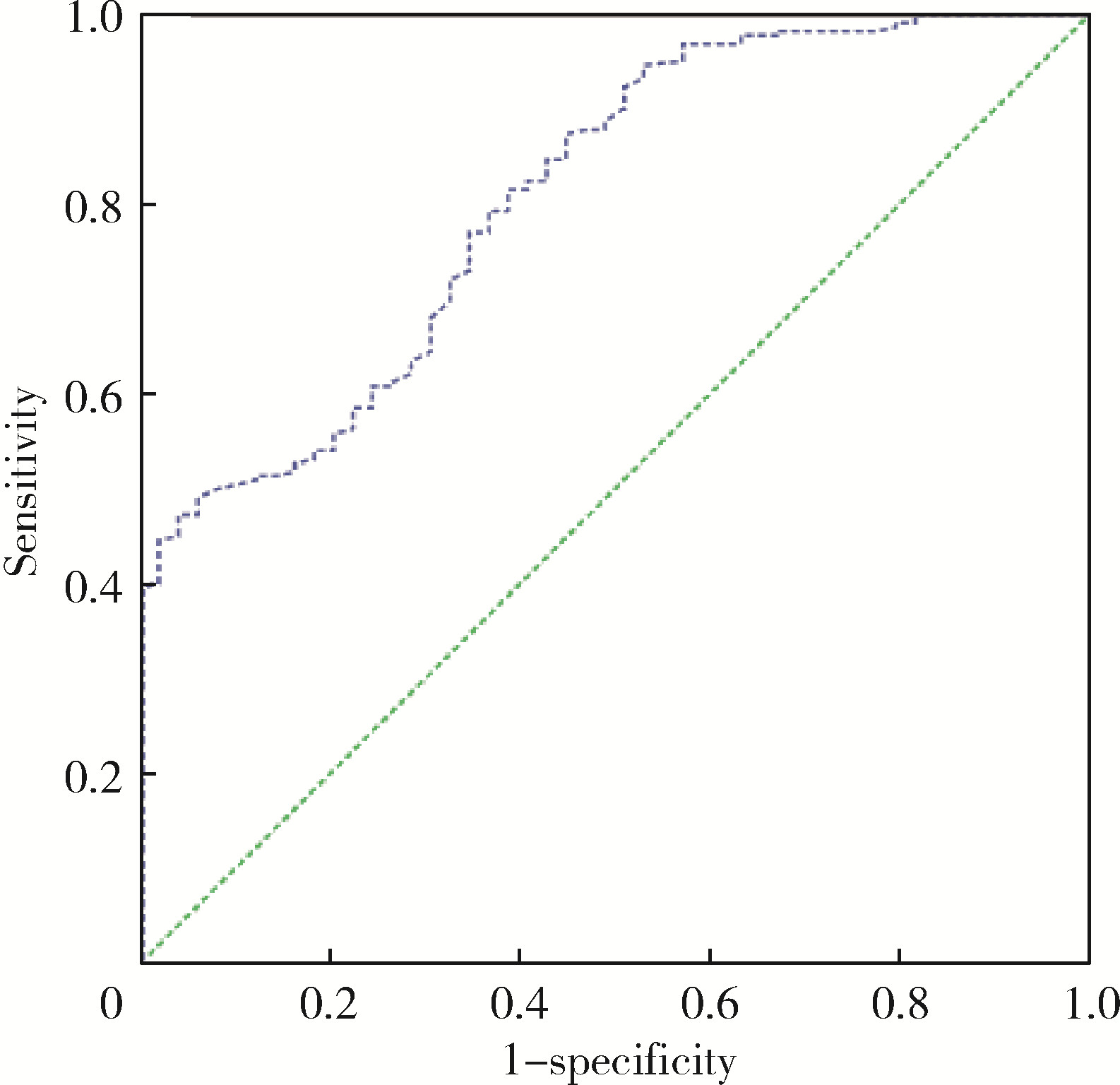
Predictive value of preoperative pelvic floor electrophysiological parameters on early urinary incontinence following radical prostatectomy
Shuhui YU1,Jianing HAN1,2,Lijun ZHONG1,Congyu CHEN1,Yunxiang XIAO1,Yanbo HUANG1,Yang YANG1,*( ),Xinyan CHE1,*()
),Xinyan CHE1,*()
- 1. Department of Urology, Peking University First Hospital, Beijing 100034, China
2. School of Nursing, Peking University, Beijing 100191, China
CLC Number:
- R737.25
| 1 |
赫捷, 陈万青, 李霓, 等. 中国前列腺癌筛查与早诊早治指南(2022, 北京)[J]. 中国肿瘤, 2022, 31 (1): 1- 30.
doi: 10.3969/j.issn.1674-4136.2022.01.001 |
| 2 |
Zhu Y , Mo M , Wei Y , et al. Epidemiology and genomics of prostate cancer in Asian men[J]. Nat Rev Urol, 2021, 18 (5): 282- 301.
doi: 10.1038/s41585-021-00442-8 |
| 3 |
Mottet N , Bellmunt J , Bolla M , et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: Screening, diagnosis, and local treatment with curative intent[J]. Eur Urol, 2017, 71 (4): 618- 629.
doi: 10.1016/j.eururo.2016.08.003 |
| 4 |
Ficarra V , Novara G , Rosen RC , et al. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy[J]. Eur Urol, 2012, 62 (3): 405- 417.
doi: 10.1016/j.eururo.2012.05.045 |
| 5 |
Abdollah F , Sun M , Suardi N , et al. Prediction of functional outcomes after nerve-sparing radical prostatectomy: Results of conditional survival analyses[J]. Eur Urol, 2012, 62 (1): 42- 52.
doi: 10.1016/j.eururo.2012.02.057 |
| 6 |
Eastham JA , Kattan MW , Rogers E , et al. Risk factors for urinary incontinence after radical prostatectomy[J]. J Urol, 1996, 156 (5): 1707- 1713.
doi: 10.1016/S0022-5347(01)65488-0 |
| 7 |
Sandhu J S , Breyer B , Comiter C , et al. Incontinence after prostate treatment: AUA/SUFU guideline[J]. J Urol, 2019, 202 (2): 369- 378.
doi: 10.1097/JU.0000000000000314 |
| 8 |
Levy A , Fleishman A , Jackson M , et al. Using preoperative pelvic floor assessment to predict early return of continence after robotic radical prostatectomy[J]. Urology, 2021, 155, 160- 164.
doi: 10.1016/j.urology.2021.04.029 |
| 9 |
Kubo Y , Tanaka K , Yamasaki M , et al. Influences of the charlson comorbidity index and nutrition status on prognosis after esophageal cancer surgery[J]. Ann Surg Oncol, 2021, 28 (12): 7173- 7182.
doi: 10.1245/s10434-021-09779-1 |
| 10 |
Jeong S J , Yeon J S , Lee J K , et al. Development and validation of nomograms to predict the recovery of urinary continence after radical prostatectomy: Comparisons between immediate, early, and late continence[J]. World J Urol, 2014, 32 (2): 437- 444.
doi: 10.1007/s00345-013-1127-y |
| 11 |
Collette ERP , Klaver SO , Lissenberg-Witte BI , et al. Patient reported outcome measures concerning urinary incontinence after robot assisted radical prostatectomy: Development and validation of an online prediction model using clinical parameters, lower urinary tract symptoms and surgical experience[J]. J Robot Surg, 2021, 15 (4): 593- 602.
doi: 10.1007/s11701-020-01145-9 |
| 12 |
Ali M , Hutchison DD , Ortiz NM , et al. A narrative review of pelvic floor muscle training in the management of incontinence following prostate treatment[J]. Transl Androl Urol, 2022, 11 (8): 1200- 1209.
doi: 10.21037/tau-22-143 |
| 13 | Hoyland K , Vasdev N , Abrof A , et al. Post-radical prostatectomy incontinence: Etiology and prevention[J]. Rev Urol, 2014, 16 (4): 181- 188. |
| 14 |
Mungovan SF , Carlsson SV , Gass GC , et al. Preoperative exercise interventions to optimize continence outcomes following radical prostatectomy[J]. Nat Rev Urol, 2021, 18 (5): 259- 281.
doi: 10.1038/s41585-021-00445-5 |
| 15 |
Laycock J , Jerwood D . Pelvic floor muscle assessment: The PERFECT scheme[J]. Physiotherapy, 2001, 87 (12): 631- 642.
doi: 10.1016/S0031-9406(05)61108-X |
| 16 |
Manassero F , Traversi C , Ales V , et al. Contribution of early intensive prolonged pelvic floor exercises on urinary continence recovery after bladder neck-sparing radical prostatectomy: Results of a prospective controlled randomized trial[J]. Neurourol Urodyn, 2007, 26 (7): 985- 989.
doi: 10.1002/nau.20442 |
| 17 |
Stanford JL , Feng Z , Hamilton AS , et al. Urinary and sexual function after radical prostatectomy for clinically localized prostate cancer: The prostate cancer outcomes study[J]. JAMA, 2000, 283 (3): 354- 360.
doi: 10.1001/jama.283.3.354 |
| 18 |
Strasser H , Tiefenthaler M , Steinlechner M , et al. Urinary incontinence in the elderly and age-dependent apoptosis of rhabdosphincter cells[J]. Lancet, 1999, 354 (9182): 918- 919.
doi: 10.1016/S0140-6736(99)02588-X |
| 19 |
Heesakkers J , Farag F , Bauer RM , et al. Pathophysiology and contributing factors in postprostatectomy incontinence: A review[J]. Eur Urol, 2017, 71 (6): 936- 944.
doi: 10.1016/j.eururo.2016.09.031 |
| [1] | Ruilin GUO, Lei ZHANG, Yu WANG, Xiaoqing WANG, Xiaoxiao WANG, Songwen NIAN, Lihui ZHANG, Bingbing XIAO, Ye LU. Effect of TVT-Abbrevo in the treatment of female stress urinary incontinence [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 337-341. |
| [2] | Qi WANG, Hanwei KE, Zehua DING, Weiyu ZHANG, Xiaopeng ZHANG, Tao XU, Kexin XU. Effects of retropubic and obturator urethral suspension on postoperative maximum flow rate and residual urine volume [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 717-720. |
| [3] | Yuqing LI,Biao WANG,Peng QIAO,Wei WANG,Xing GUAN. Medium to long-term efficacy of tension-free vaginal tape procedure in the treatment of female recurrent stress urinary incontinence [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 600-604. |
| [4] | Ye YAN,Xiaolong LI,Haizhui XIA,Xuehua ZHU,Yuting ZHANG,Fan ZHANG,Ke LIU,Cheng LIU,Lulin MA. Analysis of risk factors for long-term overactive bladder after radical prostatectomy [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 589-593. |
| [5] | ZHANG Fan,CHEN Qu,HAO Yi-chang,YAN Ye,LIU Cheng,HUANG Yi,MA Lu-lin. Relationship between recovery of urinary continence after laparoscopic radical prostatectomy and preoperative/postoperative membranous urethral length [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 299-303. |
| [6] | HAO Han,LIU Yue,CHEN Yu-ke,SI Long-mei,ZHANG Meng,FAN Yu,ZHANG Zhong-yuan,TANG Qi,ZHANG Lei,WU Shi-liang,SONG Yi,LIN Jian,ZHAO Zheng,SHEN Cheng,YU Wei,HAN Wen-ke. Evaluating continence recovery time after robot-assisted radical prostatectomy [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 697-703. |
| [7] | ZHANG Fan,HUANG Xiao-juan,YANG Bin,YAN Ye,LIU Cheng,ZHANG Shu-dong,HUANG Yi,MA Lu-lin. Relationship between prostate apex depth and early recovery of urinary continence after laparoscopic radical prostatectomy [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 692-696. |
| [8] | Xin-yan CHE,Shi-liang WU,Yu-ke CHEN,Yan-bo HUANG,Yang YANG. A survey of risk factors and quality of life in female medical staff with urinary incontinence [J]. Journal of Peking University(Health Sciences), 2019, 51(4): 706-710. |
| [9] | Xian-hui LIU,Wei-yu ZHANG,Hao HU,Qi WANG,Tao WANG,Yong-xin HE,Ke-xin XU. Long-term follow-up of the efficacy of tension-free vaginal tape and trans-obturator tape for different types of stress urinary incontinence [J]. Journal of Peking University(Health Sciences), 2019, 51(4): 694-697. |
| [10] | ZHANG Wei-yu, ZHANG Xiao-peng, HU Hao, CHEN Jing-wen, LIU Xian-hui, XU Ke-xin. Analysis of outcomes of tension-free mid-urethral sling procedure in women with mixed urinary incontinence [J]. Journal of Peking University(Health Sciences), 2017, 49(4): 638-642. |
| [11] | ZHANG Wei-yu, ZHANG Xiao-peng, CHEN Jing-wen, SUN Yi-ran, WANG Jia, HU Hao, XU Ke-xin. Effect of age on urodynamic parameters of women with urinary incontinence [J]. Journal of Peking University(Health Sciences), 2016, 48(5): 825-829. |
| [12] | ZHANG Wei-yu, HU Hao, WANG Qi, CHEN Jing-wen, XU Ke-xin. Significance of preoperative urodynamics for clinical diagnosis of female patients with stress urinary incontinence [J]. Journal of Peking University(Health Sciences), 2016, 48(4): 655-658. |
| [13] | LIAO Xiao-Xing, XING Nian-Zeng, QIAO Peng, KANG Ning, ZHANG Jun-Hui, NIU Yi-Nong. "Sandwich” urethra reconstruction improves the early continence following laparoscopic radical prostatectomy [J]. Journal of Peking University(Health Sciences), 2015, 47(4): 601-604. |
| [14] | JIA Xiao-Jun, FANG Zhi-Wei, HU Hao, XU Ke-Xin, HUANG Xiao-Bo, WANG Xiao-Feng. Influence of tension-free midurethral sling surgery on sexual function in women with stress urinary incontinence [J]. Journal of Peking University(Health Sciences), 2014, 46(4): 570-573. |
|
||