Journal of Peking University(Health Sciences) ›› 2019, Vol. 51 ›› Issue (4): 769-774. doi: 10.19723/j.issn.1671-167X.2019.04.031
Previous Articles Next Articles
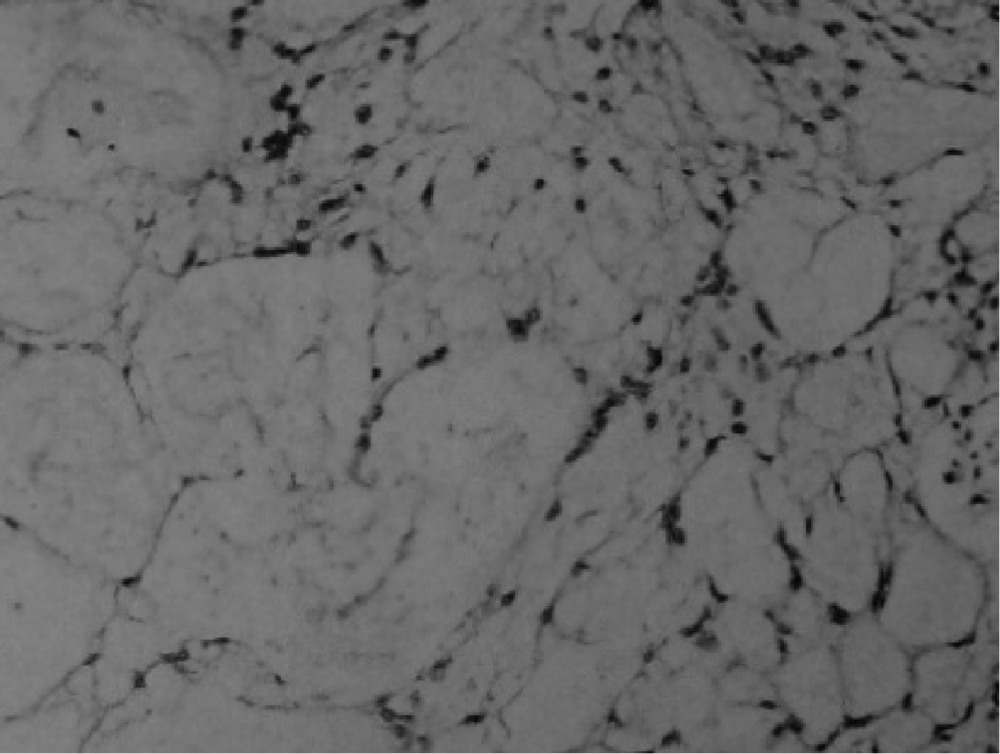
Superficial siderosis of the central nervous system caused by myxopapillary ependymoma of conus medullaris and cauda equine: a case report and literature review
Li XU1,Ming-jie HU2,Yu-yu LI1,Hong-dang QU1,Wei-dong QIAN1,Xiao-lin LIU1,△( )
)
- 1. Department of Neurology, The First Affiliated Hospital of Bengbu Medical College, Bengbu 233004, Anhui, China
2. School of Life Sciences, Bengbu Medical College, Bengbu 233020, Anhui, China
CLC Number:
- R739.4

| [1] | Wang K, Xu Z, Xiong G , et al. Superficial siderosis of the central nervous system manifested with seizures[J]. J Clin Neurosci, 2010,17(2):277-278. |
| [2] | Levy M, Turtzo C, Llinas RH . Superficial siderosis: a case report and review of the literature[J]. Nat Clin Pract Neurol, 2007,3(1):54-58. |
| [3] | Sydlowski SA, Cevette MJ, Shallop J . Superficial siderosis of the central nervous system: phenotype and implications for audiology and otology[J]. Otol Neurotol, 2011,32(6):900-908. |
| [4] | Savoiardo M, Grisoli M . Further in-depth look at superficial side-rosis (and intracranial hypotension)[J]. AJNR Am J Neurora-diol, 2010,31(8):E72-E73. |
| [5] | Rodriguez FR, Srinivasan A . Superficial siderosis of the CNS[J]. AJR Am J Roentgenol, 2011,197(1):W149-W152. |
| [6] | Wang J, Gong X . Superficial siderosis of the central nervous system: MR findings with susceptibility-weighted imaging[J]. Clin Imaging, 2011,35(3):217-221. |
| [7] | Kumar N . Neuroimaging in superficial siderosis: an in-depth look[J]. AJNR Am J Neuroradiol, 2010,31(1):5-14. |
| [8] | Khalatbari K . Case 141: superficial siderosis[J]. Radiology, 2009,250(1):292-297. |
| [9] | Koeppen AH, Michael SC, Li D , et al. The pathology of superficial siderosis of the central nervous system[J]. Acta Neuropathol, 2008,116(4):371-382. |
| [10] | Tosaka M, Sato K, Amanuma M , et al. Superficial siderosis of the central nervous system caused by hemorrhagic intraventricular craniopharyngioma: case report and literature review[J]. Neurol Med Chir (Tokyo), 2015,55(1):89-94. |
| [11] | Friedman DP, Hollander MD . Neuroradiology case of the day. Myxopapillary ependymoma of the conus medullaris or filum terminale resulting in superficial siderosis and dissemination of tumor along CSF pathways[J]. Radiographics, 1998,18(3):794-798. |
| [12] | Lemmerling M, De Praeter G, Mollet P , et al. Secondary superficial siderosis of the central nervous system in a patient presenting with sensorineural hearing loss[J]. Neuroradiology, 1998,40(5):312-314. |
| [13] | Messori A, Di Bella P, Herber N , et al. The importance of suspecting superficial siderosis of the central nervous system in clinical practice[J]. J Neurol Neurosurg Psychiatry, 2004,75(2):188-190. |
| [14] | Spengos K, Vassilopoulou S, Tsivgoulis G , et al. Superficial siderosis due to a lumbar ependymoma mimicking adult-onset spinocerebellar ataxia[J]. Clin Neurol Neurosurg, 2007,109(8):705-707. |
| [15] | Grech R, Galvin L, Looby S , et al. Spinal ependymoma complicated by superficial siderosis [J]. BMJ Case Rep, 2013: pii: bcr2013201036. doi: 10.1136/bcr-2013-201036. |
| [16] | Pikis S, Cohen JE, Vargas AA , et al. Superficial siderosis of the central nervous system secondary to spinal ependymoma[J]. J Clin Neurosci, 2014,21(11):2017-2019. |
| [17] | Ulrich CT, Beck J, Seifert V , et al. Ependymoma of conus medullaris presenting as subarachnoid haemorrhage[J]. Acta Neurochir (Wien), 2008,150(2):185-188 |
| [18] | Argyropoulou PI, Argyropoulou MI, Tsampoulas C , et al. Myxopapillary ependymoma of the conus medullaris with subarachnoid haemorrhage: MRI in two cases[J]. Neuroradiology, 2001,43(6):489-491. |
| [19] | Busche K . Neurologic disorders associated with weight lifting and body building[J]. Neurol Clin, 2008,26(1):309-324. |
| [20] | Khalatbari MR, Moharamzad Y . Myxopapillary ependymoma of the conus medullaris presenting with intratumoral hemorrhage during weight lifting in a teenager Childs[J]. Nerv Syst, 2014,30(1):181-183. |
| [21] | Boncoraglio GB, Ballabio E, Erbetta A , et al. Superficial siderosis due to dural defect with thoracic spinal cord herniation[J]. J Neurol Sci, 2012,312(1-2):170-172. |
| [22] | Levy M, Llinas RH . Update on a patient with superficial siderosis on deferiprone[J]. AJNR Am J Neuroradiol, 2012,33(6):E99-E100. |
| [1] | Zeyuan WANG, Shuanbao YU, Haoke ZHENG, Jin TAO, Yafeng FAN, Xuepei ZHANG. A preoperative prediction model for pelvic lymph node metastasis in prostate cancer: Integrating clinical characteristics and multiparametric MRI [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 684-691. |
| [2] | Jianjun SUN, Qianquan MA, Xiaoliang YIN, Chenlong YANG, Jia ZHANG, Suhua CHEN, Chao WU, Jingcheng XIE, Yunfeng HAN, Guozhong LIN, Yu SI, Jun YANG, Haibo WU, Qiang ZHAO. Significance of precise classification of sacral meningeal cysts by multiple dimensions radiographic reconstruction MRI in guiding operative strategy and rehabilitation [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 303-308. |
| [3] | Yuxuan TIAN,Mingjian RUAN,Yi LIU,Derun LI,Jingyun WU,Qi SHEN,Yu FAN,Jie JIN. Predictive effect of the dual-parametric MRI modified maximum diameter of the lesions with PI-RADS 4 and 5 on the clinically significant prostate cancer [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 567-574. |
| [4] | Yi LIU,Chang-wei YUAN,Jing-yun WU,Qi SHEN,Jiang-xi XIAO,Zheng ZHAO,Xiao-ying WANG,Xue-song LI,Zhi-song HE,Li-qun ZHOU. Diagnostic efficacy of prostate cancer using targeted biopsy with 6-core systematic biopsy for patients with PI-RADS 5 [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 812-817. |
| [5] | Chang-wei YUAN,De-run LI,Zhi-hua LI,Yi LIU,Gang-zhi SHAN,Xue-song LI,Li-qun ZHOU. Application of dynamic contrast enhanced status in multiparametric magnetic resonance imaging for prostatic cancer with PI-RADS 4 lesion [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 838-842. |
| [6] | Ying LIU,Ran HUO,Hui-min XU,Zheng WANG,Tao WANG,Hui-shu YUAN. Correlations between plaque characteristics and cerebral blood flow in patients with moderate to severe carotid stenosis using magnetic resonance vessel wall imaging [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 646-651. |
| [7] | Qiang FU,Guan-ying GAO,Yan XU,Zhuo-hua LIN,You-jing SUN,Li-gang CUI. Comparative study of ultrasound and magnetic resonance imaging in the diagnosis of asymptomatic anterosuperior acetabular labrum tears [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 665-669. |
| [8] | Shan YE,Ping-ping JIN,Nan ZHANG,Hai-bo WU,Lin SHI,Qiang ZHAO,Kun YANG,Hui-shu YUAN,Dong-sheng FAN. Cortical thickness and cognitive impairment in patients with amyotrophic lateral sclerosis [J]. Journal of Peking University (Health Sciences), 2022, 54(6): 1158-1162. |
| [9] | Ying CAI,Qiao-qin WAN,Xian-jie CAI,Ya-juan GAO,Hong-bin HAN. Epidural photobiomodulation accelerates the drainage of brain interstitial fluid and its mechanism [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 1000-1005. |
| [10] | WANG Shu-lei,GAO Yang-xu,ZHANG Hong-wu,YANG Hai-bo,LI Hui,LI Yu,SHEN Li-xue,YAO Hong-xin. Clinical analysis of 30 cases of basal ganglia germinoma in children [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 222-226. |
| [11] | ZHANG Fan,CHEN Qu,HAO Yi-chang,YAN Ye,LIU Cheng,HUANG Yi,MA Lu-lin. Relationship between recovery of urinary continence after laparoscopic radical prostatectomy and preoperative/postoperative membranous urethral length [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 299-303. |
| [12] | Yi-fan WU,Xiao-yuan ZHANG,Shuang REN,Ying-xiang YU,Cui-qing CHANG. Measurement and evaluation of the quadriceps muscle mass in young men based on magnetic resonance imaging [J]. Journal of Peking University (Health Sciences), 2021, 53(5): 843-849. |
| [13] | Hui SHENG,Lei LIANG,Tong-liang ZHOU,Yan-xing JIA,Tong WANG,Lan YUAN,Hong-bin HAN. Improved synthesis process of optical-magnetic bimodal probe of Gd-[4,7-Bis-carboxymethyl-10-(2-fluoresceinthioureaethyl)-1,4,7,10-tetraaza-cyclododec-1-yl]-acetic acid complexes [J]. Journal of Peking University (Health Sciences), 2020, 52(5): 959-963. |
| [14] | Shi-ming ZHAO,Tie-jun YANG,Chun-miao XU,Xiao-feng GUO,Yong-kang MA,Xue-jun CHEN,Xiang LI,Chao-hong HE. Bladder cancer local staging about muscle invasion: 3.0T MRI performance following transurethral resection [J]. Journal of Peking University (Health Sciences), 2020, 52(4): 701-704. |
| [15] | Yu SONG,Hong-bin HAN,Jun YANG,Ai-bo WANG,Qing-yuan HE,Yuan-yuan LI,Guo-mei ZHAO,Ya-juan GAO,Rui WANG,Yi-xing HAN,Ai-lian LIU,Qing-wei SONG. Effect of convection enhanced delivery on the microstructure of brain extracellular space in aged rats [J]. Journal of Peking University (Health Sciences), 2020, 52(2): 362-367. |
|
||