Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (3): 460-466. doi: 10.19723/j.issn.1671-167X.2021.03.004
Previous Articles Next Articles
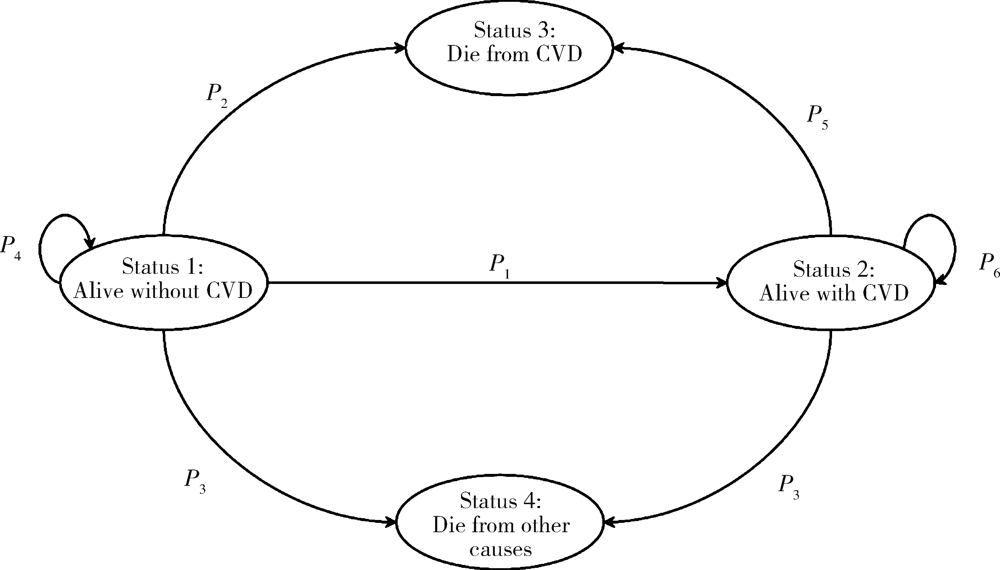
Effectiveness of different screening strategies for cardiovascular diseases prevention in a community-based Chinese population: A decision-analytic Markov model
LIU Qiu-ping1,CHEN Xi-jin2,WANG Jia-min1,LIU Xiao-fei2,SI Ya-qin1,LIANG Jing-yuan1,SHEN Peng3,LIN Hong-bo3,TANG Xun1,Δ( ),GAO Pei1,2,Δ()
),GAO Pei1,2,Δ()
- 1. Department of Epidemiology and Biostatistics, Peking University School of Public Health, Beijing 100191, China
2. Center for Real-world Evidence Evaluation, Peking University Clinical Research Institute, Beijing 100191, China
3. Yinzhou District Center for Disease Control and Prevention, Ningbo 315101, Zhejiang, China
CLC Number:
- R181.32

| [1] | Owen AJ, Reid CM. Systematic versus opportunistic risk assessment for the primary prevention of cardiovascular disease[J]. Cochrane Database Syst Rev, 2016,2016(1): CD010411. |
| [2] |
Brainin M, Sliwa K. WSO and WHF joint position statement on population-wide prevention strategies[J]. Lancet, 2020,396(10250):533-534.
doi: 10.1016/S0140-6736(20)31752-9 |
| [3] | 中国心血管病风险评估和管理指南编写联合委员会. 中国心血管病风险评估和管理指南[J]. 中华预防医学杂志, 2019,53(1):13-35. |
| [4] | 中华医学会心血管病学分会, 中国康复医学会心脏预防与康复专业委员会, 中国老年学和老年医学会心脏专业委员会, 等. 中国心血管病一级预防指南[J]. 中华心血管病杂志, 2020,48(12):1000-1038. |
| [5] |
Xu G, Ma M, Liu X, et al. Is there a stroke belt in China and why?[J]. Stroke, 2013,44(7):1775-1783.
doi: 10.1161/STROKEAHA.113.001238 |
| [6] | 司亚琴, 唐迅, 张杜丹, 等. 北方农村人群心血管病一级预防筛查策略的评价[J]. 北京大学学报(医学版), 2018,50(3):443-449. |
| [7] | 刘秋萍, 高培, 唐迅, 等. 马尔可夫模型在流行病学筛查成本效果分析中的应用[J]. 中华流行病学杂志, 2021,42(4):728-734. |
| [8] |
Gu D, He J, Coxson PG, et al. The cost-effectiveness of low-cost essential antihypertensive medicines for hypertension control in China: A modelling study[J]. PLoS Med, 2015,12(8):e1001860.
doi: 10.1371/journal.pmed.1001860 |
| [9] |
Lin H, Tang X, Shen P, et al. Using big data to improve cardiovascular care and outcomes in China: A protocol for the Chinese electronic health records research in Yinzhou (CHERRY) study[J]. BMJ Open, 2018,8(2):e019698.
doi: 10.1136/bmjopen-2017-019698 |
| [10] |
Zhang D, Tang X, Shen P, et al. Multimorbidity of cardiometabolic diseases: Prevalence and risk for mortality from one million Chinese adults in a longitudinal cohort study[J]. BMJ Open, 2019,9(3):e024476.
doi: 10.1136/bmjopen-2018-024476 |
| [11] | Ma C, Avenell A, Bolland M, et al. Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: Systematic review and meta-analysis[J]. BMJ, 2017,359:j4849. |
| [12] |
Tan CE, Glantz SA. Association between smoke-free legislation and hospitalizations for cardiac, cerebrovascular, and respiratory diseases: A meta-analysis[J]. Circulation, 2012,126(18):2177-2183.
doi: 10.1161/CIRCULATIONAHA.112.121301 |
| [13] |
Lim SH, Tai BC, Yuan JM, et al. Smoking cessation and mortality among middle-aged and elderly Chinese in Singapore: the Singapore Chinese health study[J]. Tob Control, 2013,22(4):235-240.
doi: 10.1136/tobaccocontrol-2011-050106 pmid: 22170337 |
| [14] | Adler AJ, Taylor F, Martin N, et al. Reduced dietary salt for the prevention of cardiovascular disease[J]. Cochrane Database Syst Rev, 2014,2014(12): CD009217. |
| [15] |
Yusuf S, Lonn E, Pais P, et al. Blood-pressure and cholesterol lowering in persons without cardiovascular disease[J]. N Engl J Med, 2016,374(21):2032-2043.
doi: 10.1056/NEJMoa1600177 |
| [16] |
Shah AD, Langenberg C, Rapsomaniki E, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1.9 million people[J]. Lancet Diabetes Endocrinol, 2015,3(2):105-113.
doi: 10.1016/S2213-8587(14)70219-0 |
| [17] |
Emerging Risk Factors Collaboration, Di Angelantonio E, Kaptoge S, et al. Association of cardiometabolic multimorbidity with mortality[J]. JAMA, 2015,314(1):52-60.
doi: 10.1001/jama.2015.7008 pmid: 26151266 |
| [18] | Kypridemos C, Allen K, Hickey G L, et al. Cardiovascular screening to reduce the burden from cardiovascular disease: Microsimulation study to quantify policy options[J]. BMJ, 2016,353:i2793. |
| [19] | 中国心血管病预防指南(2017)写作组, 中华心血管病杂志编辑委员会. 中国心血管病预防指南(2017)[J]. 中华心血管病杂志, 2018,46(1):10-25. |
| [20] |
Matsushita K, Coresh J, Sang Y, et al. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: A collaborative meta-analysis of individual participant data[J]. Lancet Diabetes Endocrinol, 2015,3(7):514-525.
doi: 10.1016/S2213-8587(15)00040-6 pmid: 26028594 |
| [21] |
Li X, Wu C, Lu J, et al. Cardiovascular risk factors in China: A nationwide population-based cohort study[J]. Lancet Public Health, 2020,5(12):e672-e681.
doi: 10.1016/S2468-2667(20)30191-2 |
| [22] |
Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines[J]. Circulation, 2019,140(11):e596-e646.
doi: 10.1161/CIR.0000000000000678 |
| [1] | Mingjia YANG, Jiangxue WU, Jing WANG, Yang LIU, Zhongmin LI, Jingjing LI, Hongtian LI, Yubo ZHOU, Jianmeng LIU. A population-based survey of myopia on primary school students in an administrative district, 2019 to 2024 [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 513-519. |
| [2] | Shang XIE, Luming WANG, Xinyuan ZHANG, Qiushi FENG, Yangyang XIA, Ziwei DAI, Xiaofeng SHAN, Zhigang CAI. Construction and application of oral squamous cell carcinoma organoid bank [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 847-851. |
| [3] | Tianjing ZHOU,Qiuping LIU,Minglu ZHANG,Xiaofei LIU,Jiali KANG,Peng SHEN,Hongbo LIN,Xun TANG,Pei GAO. Comparison of initiation of antihypertensive therapy strategies for primary prevention of cardiovascular diseases in Chinese population: A decision-analytic Markov modelling study [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 441-447. |
| [4] | Ming-lu ZHANG,Qiu-ping LIU,Chao GONG,Jia-min WANG,Tian-jing ZHOU,Xiao-fei LIU,Peng SHEN,Hong-bo LIN,Xun TANG,Pei GAO. Comparison of aspirin treatment strategies for primary prevention of cardiovascular diseases: A decision-analytic Markov modelling study [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 480-487. |
| [5] | Jia-min WANG,Qiu-ping LIU,Ming-lu ZHANG,Chao GONG,Shu-dan LIU,Wei-ye CHEN,Peng SHEN,Hong-bo LIN,Pei GAO,Xun TANG. Effectiveness of different screening strategies for type 2 diabete on preventing cardiovascular diseases in a community-based Chinese population using a decision-analytic Markov model [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 450-457. |
| [6] | Chao GONG, Qiu-ping LIU, Jia-min WANG, Xiao-fei LIU, Ming-lu ZHANG, Han YANG, Peng SHEN, Hong-bo LIN, Xun TANG, Pei GAO. Effectiveness of statin treatment strategies for primary prevention of cardiovascular diseases in a community-based Chinese population: A decision-analytic Markov model [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 443-449. |
| [7] | GUO Zi-ning, LIANG Zhi-sheng, ZHOU Yi, ZHANG Na, HUANG Jie. Genetic study of cardiovascular disease subtypes defined by International Classification of Diseases [J]. Journal of Peking University (Health Sciences), 2021, 53(3): 453-459. |
| [8] | Jia-li CHEN,Yue-bo JIN,Yi-fan WANG,Xiao-ying ZHANG,Jing LI,Hai-hong YAO,Jing HE,Chun LI. Clinical characteristics and risk factors of cardiovascular disease in patients with elderly-onset rheumatoid arthritis: A large cross-sectional clinical study [J]. Journal of Peking University (Health Sciences), 2020, 52(6): 1040-1047. |
| [9] | Le GAO,Shu-qing YU,Ji-chun YANG,Jun-ling MA,Si-yan ZHAN,Feng SUN. Quality assessment of global guidelines on colorectal cancer screening [J]. Journal of Peking University(Health Sciences), 2019, 51(3): 548-555. |
| [10] | YANG Chao, WANG Jin-wei, YANG Yao-zheng, BAI Kun-hao, GAO Bi-xia, ZHAO Ming-hui, ZHANG Lu-xia, WU Shou-ling, WANG Fang. Impact of anemia and chronic kidney disease on the risk of cardiovascular disease and all-cause mortality among diabetic patients [J]. Journal of Peking University(Health Sciences), 2018, 50(3): 495-500. |
| [11] | SI Ya-qin, TANG Xun, ZHANG Du-dan, HE Liu, CAO Yang, WANG Jin-wei, LI Na, LIU Jian-jiang, GAO Pei, HU Yong-hua. Effectiveness of different screening strategies for primary prevention of cardiovascular diseases in a rural northern Chinese population [J]. Journal of Peking University(Health Sciences), 2018, 50(3): 443-449. |
| [12] | TANG Xun1, ZHANG Du-dan, HE Liu, CAO Yang, WANG Jin-wei, LI Na, HUANG Shao-ping, DOU Hui-dong, GAO Pei, HU Yong-hua. Application of the China-PAR risk prediction model for atherosclerotic cardiovascular disease in a rural northern Chinese population [J]. Journal of Peking University(Health Sciences), 2017, 49(3): 439-445. |
| [13] | GAO Ying, ZHU Cheng-gang, WU Na-qiong, GUO Yuan-lin, LIU Geng, DONG Qian, LI Jian-jun. Study on the reliability of CardioChek PA for measuring lipid profile [J]. Journal of Peking University(Health Sciences), 2016, 48(3): 523-528. |
| [14] | GAO Ming-Yue, YANG Min, KUANG Wei-Hong, QIU Pei-Yuan. Factors and validity analysis of Mini-Mental State Examination in Chinese elderly people [J]. Journal of Peking University(Health Sciences), 2015, 47(3): 443-449. |
| [15] | YU Yang, SHENG Qin-Hui, ZHANG Bao-Wei, DING Wen-Hui. Left atrial size predicts adverse cardiac events in patients with non-obstruction hypertrophic cardiomyopathy [J]. Journal of Peking University(Health Sciences), 2014, 46(2): 207-210. |
|
||