Journal of Peking University (Health Sciences) ›› 2022, Vol. 54 ›› Issue (3): 434-442. doi: 10.19723/j.issn.1671-167X.2022.03.007
Previous Articles Next Articles
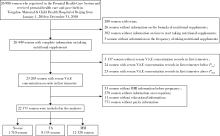
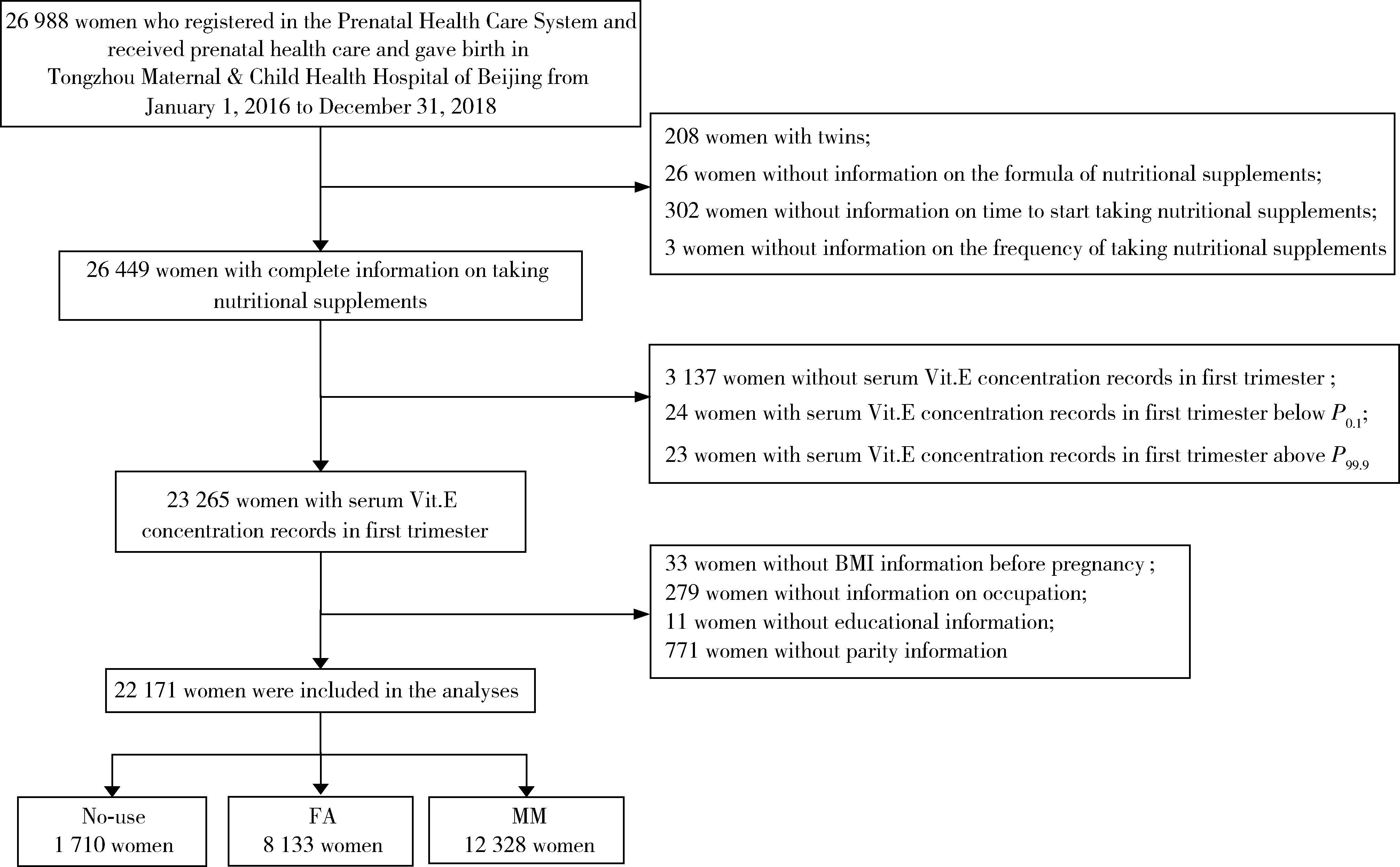
Relationship between micronutrients supplementation during periconceptional period and serum concentration of vitamin E in the 1st trimester of gestational period
Yun-fei XING1,Chun-yi LIU1,Wen-ying MENG2,Jie ZHANG1,Ming-yuan JIAO3,Lei JIN4,Lei JIN1,*( )
)
- 1. Institute of Reproductive and Child Health, Peking University; National Health Commission Key Laboratory of Reproductive Health, Beijing 100191, China
2. Department of Obstetrics, Tongzhou Maternal & Child Health Hospital of Beijing, Beijing 101100, China
3. Department of Clinical Laboratory, Tongzhou Maternal & Child Health Hospital of Beijing, Beijing 101100, China
4. Department of Maternal Health Care, Tongzhou Maternal & Child Health Hospital of Beijing, Beijing 101100, China
CLC Number:
- R169


| 1 |
Steegers-Theunissen RP , Twigt J , Pestinger V , et al. The periconceptional period, reproduction and long-term health of offspring: The importance of one-carbon metabolism[J]. Hum Reprod Update, 2013, 19 (6): 640- 655.
doi: 10.1093/humupd/dmt041 |
| 2 | Chen H , Qian N , Yan L , et al. Role of serum vitamin A and E in pregnancy[J]. Exp Ther Med, 2018, 16 (6): 5185- 5189. |
| 3 | 李俊, 郑春梅, 倪君君, 等. 2013-2016年北京地区孕妇维生素A、维生素E营养水平[J]. 卫生研究, 2019, 48 (1): 56- 60. |
| 4 | 李浩, 倪君君, 郑春梅. 2016年我国北方地区孕妇维生素A、E营养状况调查[J]. 中国医药导报, 2019, 16 (9): 64- 67. |
| 5 | 申南, 陆娣, 郑春梅, 等. 常规保健下不同年龄段孕妇妊娠早期血清维生素A、E水平分析[J]. 中国妇产科临床杂志, 2018, 19 (4): 356- 358. |
| 6 | 贾军恒, 田文琴, 强莉. 不同孕期妇女血清维生素A、维生素E水平的临床观察[J]. 中国妇幼保健, 2019, 34 (3): 509- 511. |
| 7 | 钮慧远, 薛秀平, 仲晓慧. 2017-2018年淮安地区孕妇维生素A、维生素E水平及其影响因素[J]. 卫生研究, 2020, 49 (1): 41- 43. |
| 8 | 孟文颖, 黄琬桐, 张杰, 等. 孕早期血清维生素E水平与妊娠期高血压疾病发病风险的关系[J]. 北京大学学报(医学版), 2020, 52 (3): 470- 478. |
| 9 |
Sharifipour F , Abedi P , Ciahkal SF , et al. Serum vitamin E level and gestational diabetes mellitus: A systematic review and meta-analysis[J]. J Diabetes Metab Disord, 2020, 19 (2): 1787- 1795.
doi: 10.1007/s40200-020-00582-5 |
| 10 | 施文瑶, 施晓华, 朱晓燕, 等. 孕期血清维生素A、D、E水平与妊娠期糖尿病的相关性研究[J]. 中国卫生检验杂志, 2021, 31 (4): 473- 475. |
| 11 |
Pazdro R , Burgess JR . The role of vitamin E and oxidative stress in diabetes complications[J]. Mech Ageing Dev, 2010, 131 (4): 276- 286.
doi: 10.1016/j.mad.2010.03.005 |
| 12 |
Nourooz-Zadeh J , Rahimi A , Tajaddini-Sarmadi J , et al. Relationships between plasma measures of oxidative stress and metabo-lic control in NIDDM[J]. Diabetologia, 1997, 40 (6): 647- 653.
doi: 10.1007/s001250050729 |
| 13 | Kutbi HA , Hammouda SA . Plasma concentrations of vitamin A and E and risk of dysglycemia in first-trimester pregnant Saudi women[J]. Diabetol Metab Syndr, 2020, (12): 17. |
| 14 | 吕祺, 阴春霞, 周硕, 等. 孕妇血清维生素D和维生素E水平与妊娠期高血压疾病发生的相关性[J]. 中国妇幼保健, 2021, 36 (16): 3662- 3665. |
| 15 |
Gilboa SM , Lee KA , Cogswell ME , et al. Maternal intake of vitamin E and birth defects, national birth defects prevention study, 1997 to 2005[J]. Birth Defects Res A Clin Mol Teratol, 2014, 100 (9): 647- 657.
doi: 10.1002/bdra.23247 |
| 16 | Rigotti A . Absorption, transport, and tissue delivery of vitamin E[J]. Molecular aspects of medicine, 2007, 28 (5): 423- 436. |
| 17 |
Traber MG , Rader D , Acuff RV , et al. Vitamin E dose-response studies in humans with use of deuterated RRR-alpha-tocopherol[J]. Am J Clin Nutr, 1998, 68 (4): 847- 853.
doi: 10.1093/ajcn/68.4.847 |
| 18 |
李军生. 维生素E吸收与代谢机制的研究进展[J]. 中国现代应用药学, 2005, 22 (6): 457- 461.
doi: 10.3969/j.issn.1007-7693.2005.06.008 |
| 19 | 陈曦, 宫照龙, 沈葹. 超高效液相色谱-三重四级杆串联质谱法测定血清中维生素A和维生素E[J]. 卫生研究, 2021, 50 (2): 301- 307. |
| 20 | 金蕾, 王程, 张杰, 等. 妇女围受孕期叶酸服用情况及其对胎儿神经管缺陷的预防效果[J]. 北京大学学报(医学版), 2020, 52 (4): 719- 725. |
| 21 |
Wang L , Leng J , Liu H , et al. Association between hypertensive disorders of pregnancy and the risk of postpartum hypertension: A cohort study in women with gestational diabetes[J]. J Hum Hypertens, 2017, 31 (11): 725- 730.
doi: 10.1038/jhh.2017.46 |
| 22 | 闫明, 张雯, 刘凯波, 等. 北京地区2010-2017年增补叶酸预防神经管缺陷工作效果分析[J]. 中国优生与遗传杂志, 2019, 27 (3): 339- 341. |
| 23 |
Bian H , Tang Y , Zhou Y , et al. Demographic variations and temporal trends in prenatal use of multiple micronutrient supplements in Beijing, 2013-2017[J]. Public Health Nutr, 2021, 24 (5): 826- 833.
doi: 10.1017/S1368980020004905 |
| 24 |
Schulze KJ , Mehra S , Shaikh S , et al. Antenatal multiple micronutrient supplementation compared to iron-folic acid affects micronutrient status but does not eliminate deficiencies in a randomized controlled trial among pregnant women of rural bangladesh[J]. J Nutr, 2019, 149 (7): 1260- 1270.
doi: 10.1093/jn/nxz046 |
| 25 | Colapinto CK , O'Connor DL , Dubois L , et al. Prevalence and correlates of folic acid supplement use in Canada[J]. Health Rep, 2012, 23 (2): 39- 44. |
| [1] | Chang LIU, Zhao LI, Lei JIN, Chunyi LIU, Chunjing WANG, Jie ZHANG, Lei JIN. Association between maternal periconceptional supplementation of folic acid or multiple micronutrients containing folic acid and perinatal mortality rate [J]. Journal of Peking University (Health Sciences), 2025, 57(3): 473-480. |
| [2] | Yue WEI,Lan YAO,Xi LU,Jun WANG,Li LIN,Kun-peng LIU. Evaluation of gastric emptying after drinking carbohydrates before cesarean section by gastric ultrasonography [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1082-1087. |
| [3] | Yin-xiao BAI,Chun-yi LIU,Jie ZHANG,Wen-ying MENG,Lei JIN,Lei JIN. Association between periconceptional supplementation of folic acid or multiple-micronutrients containing folic acid and preterm delivery in women [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 495-501. |
| [4] | Lei JIN,Cheng WANG,Jie ZHANG,Wen-ying MENG,Jia-yu ZHANG,Jin-hui YU,Gui-yin LIN,Ming-kun TONG,Lei JIN. Maternal periconceptional folic acid supplementation and its effects on the prevalence of fetal neural tube defects [J]. Journal of Peking University (Health Sciences), 2020, 52(4): 719-725. |
| [5] | Wen-ying MENG,Wan-tong HUANG,Jie ZHANG,Ming-yuan JIAO,Lei JIN,Lei JIN. Relationship between serum vitamin E concentration in first trimester and the risk of developing hypertension disorders complicating pregnancy [J]. Journal of Peking University (Health Sciences), 2020, 52(3): 470-478. |
| [6] | Zhang-jian CHEN,Shuo HAN,Pai ZHENG,Shu-pei ZHOU,Guang JIA. Effect of subchronic combined oral exposure of titanium dioxide nanoparticles and glucose on levels of serum folate and vitamin B12 in young SD rats [J]. Journal of Peking University (Health Sciences), 2020, 52(3): 451-456. |
| [7] | SUN Ying, JIN Lei. Blood manganese levels among pregnant women and the associated factors in three counties of northern China [J]. Journal of Peking University(Health Sciences), 2018, 50(3): 463-468. |
| [8] | YUAN Meng-meng, WANG Meng, LIU Jun-yi, ZHANG Zhi-li. Optimization of alkaline hydrolysis based on the side chain of diethyl ester 4-amino-N5 -formyl-N8,N10 -dideazatetrahydrofolic acid [J]. Journal of Peking University(Health Sciences), 2017, 49(4): 714-718. |
| [9] | LIU Xin, DU Yi-qing, LI Yuan-xin, WANG Meng, ZHANG Zhi-li, WANG Xiao-wei, LIU Jun-yi, TIAN Chao. Improved synthesis process of diethyl N-[4-[(2,4-diaminopyrido[3,2-d]pyrimidin-6-yl)methylamino]benzoyl]-L-glutamate [J]. Journal of Peking University(Health Sciences), 2015, 47(5): 842-845. |
|
||