
1 AFPGC的分型和新临床特征
1.1 AFPGC的基因型
1.2 AFPGC并不等同于胃肝样腺癌
表1 AFPGC与HAS和HCC的区别Table 1 Differential characteristics of AFPGC, HAS and HCC |
| Features | AFPGC | HAS | HCC |
| Cellular origin | Gastric glandular epithelium | Stomach (with hepatoid differentiation) | Hepatic parenchyma |
| AFP levels[7] | Elevated (≥7 μg/L) | Elevated | Significantly elevated (pathognomonic) |
| Pathological features[8-9] | Gastric adenocarcinoma, focal hepatoid changes | Dual features of gastric adenocarcinoma and HCC | Liver malignancy, hepatoid differentiation |
| Molecular profile[10-11] | Gastric-like, TP53 (55%), CDH1 | HCC-like, TP53 (66%) | TP53, CTNNB1, TERT promoter mutations |
| ERBB2 amplification[11] | Highest (25.8%) | Intermediate (21.05%) | Lowest (0.6%) |
| Molecular/IHC markers[12-13] | AFP (+), GPC3 (64.84%) | AFP (+), GPC3 (78.1%) | AFP (+), GPC3 (+), HCC hallmarks |
| Therapeutic strategies[14] | Resection, chemo, and immunothe-rapy | Refractory to gastric cancer regimens, HCC-oriented therapy | Transplant, targeted therapy, and immunotherapy |
| Prognosis[15] | Poor, AFP elevation correlated with stage and invasiveness | Poor, especially in AFP-high cases, low 5-year survival, frequent liver metastasis | Poor, particularly in advanced stages or patients with cirrhosis |
AFPGC, alpha-fetoprotein-producing gastric cancer; HAS, hepatoid adenocarcinoma of the stomach; HCC, hepatocellular carcinoma; AFP, alpha-fetoprotein; IHC, immunohistochemistry. |
表2 AFPGC的临床分型及其AFP、VEGF、CEA表达情况[16]Table 2 Clinical subtypes and expression of AFP, VEGF, and CEA in AFPGC[16] |
| Subtype | n | AFP (+) | VEGF (+) | CEA (+) |
| Hepatoid | 19 | 7 (36.8%) | 9 (47.4%) | 7 (36.8%) |
| Yolk sac tumor-like | 32 | 7 (21.9%) | 9 (28.1%) | 24 (75.0%) |
| Fetal gastrointestinal | 5 | 0 (0) | 1 (20.0%) | 4 (80.0%) |
| Mixed | 8 | 1 (12.5%) | 2 (25.0%) | 7 (87.5%) |
AFPGC, alpha-fetoprotein-producing gastric cancer; AFP, alpha-fetoprotein; VEGF, vascular endothelial growth factor; CEA, carcinoembryonic antigen. |
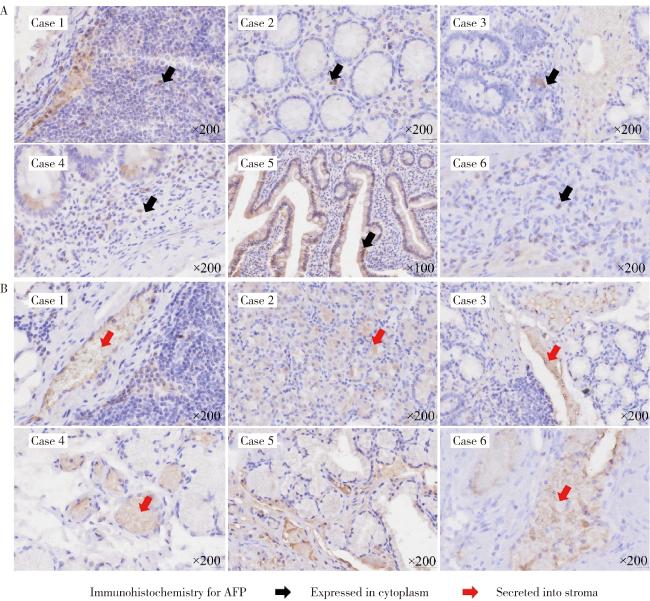
1.3 AFPGC患者的AFP蛋白可以不出现在外周血,仅在胃癌组织中表达
1.4 AFPGC具有独特的生物学特性及基因突变和染色体异常特征
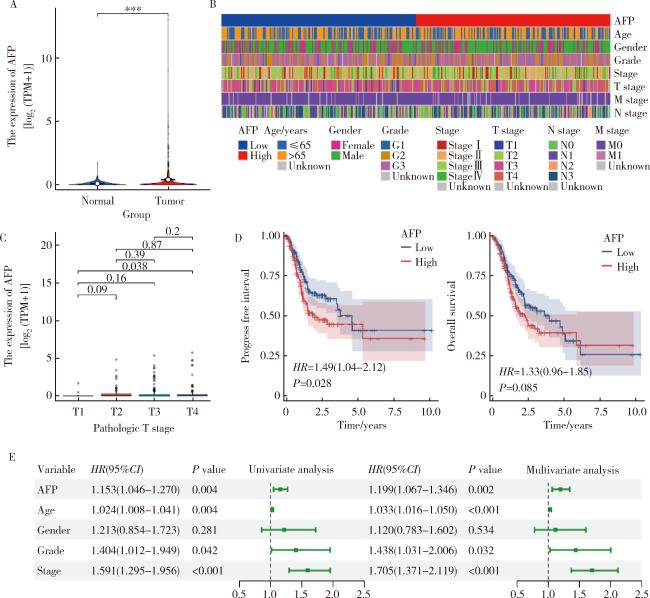
图2 AFP在胃癌预后中的作用Figure 2 Prognostic role of AFP expression in gastric cancer A, comparison of AFP mRNA levels between normal and tumor tissues; B, heatmap correlating AFP expression (high vs. low) with key clinicopatho-logical features; C, correlation between AFP expression and pathologic T stage; D, Kaplan-Meier curves for progress-free survival (PFS) and overall survival (OS); E, integrated forest plot of univariate and multivariate Cox regression analyses. AFP, alpha-fetoprotein. |
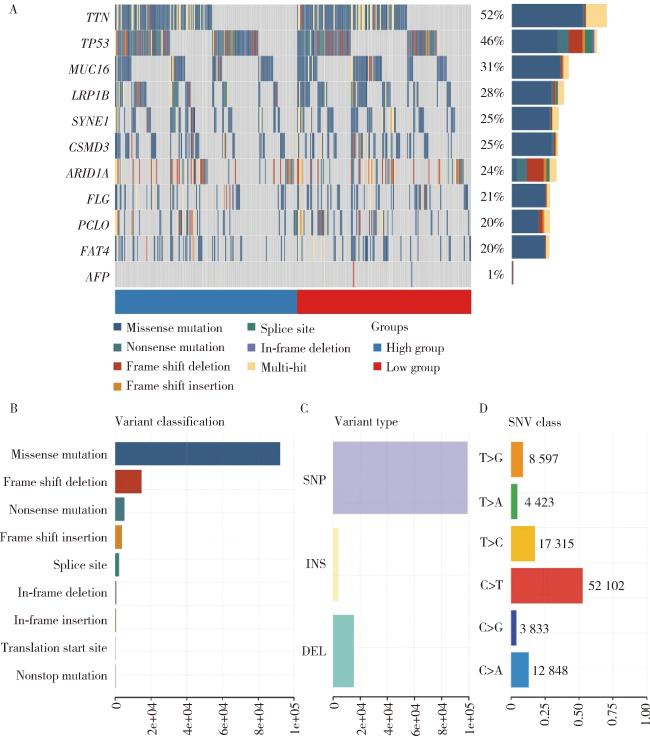
图3 AFP高表达的胃癌中基因突变情况Figure 3 Genomic mutation landscape in gastric cancer with high AFP expression A, oncoplot of mutated genes; B, summary of variant classifications; C, distribution of variant types; D, profiling of SNV classes. AFP, alpha-fetoprotein; SNV, single nucleotide variant; SNP, single nucleotide polymorphism; INS, insertion; DEL, deletion. |
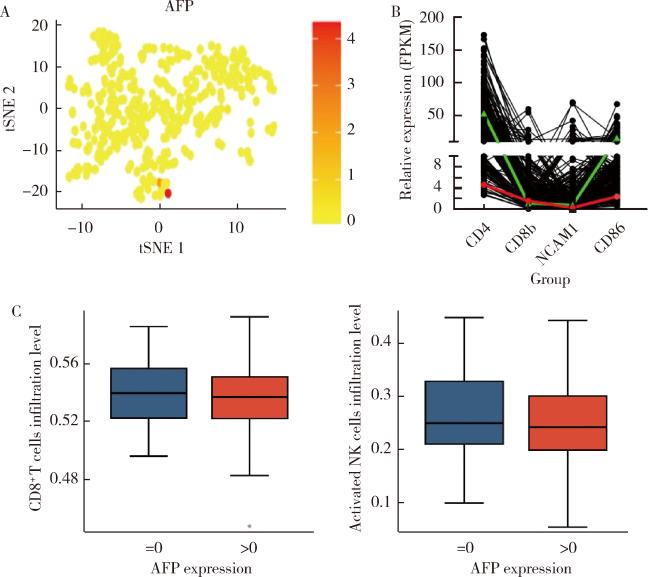
图4 胃癌中AFP表达与免疫浸润的关系Figure 4 Correlation between AFP expression and immune infiltration in gastric cancer A, tSNE visualization of AFP expression; B, relative expression levels of immune-related markers; C, infiltration levels of CD8+ T cells and activated NK cells stratified by AFP expression status. NK, natural killer cell; AFP, alpha-fetoprotein; FPKM, fragments per kilobase of exon model per million mapped fragments; tSNE, t-distributed stochastic neighbor embedding. |
2 一些值得临床关注的AFPGC特殊亚型
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
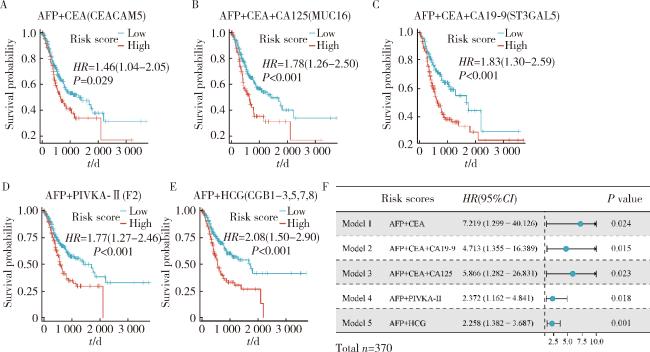
图5 AFPGC特殊亚型的预后分析Figure 5 Prognostic value of multi-biomarker models in AFPGC A-E, Kaplan-Meier survival curves illustrating risk-stratified overall survival outcomes based on various biomarker combinations; F, forest plot summarizing the hazard ratio (HR) and 95% confidence interval (CI) for five multivariate Cox regression analysis. All Cox regression models were adjusted for age, gender, tumor grade, and pathologic stage. AFPGC, alpha-fetoprotein-producing gastric cancer; AFP, alpha-fetoprotein; CEA, carcinoembryonic antigen; HCG, human chorionic gonadotropin; PIVKA-Ⅱ, protein induced by vitamin K absence or antagonist-Ⅱ. |