
1 资料与方法
1.1 研究对象
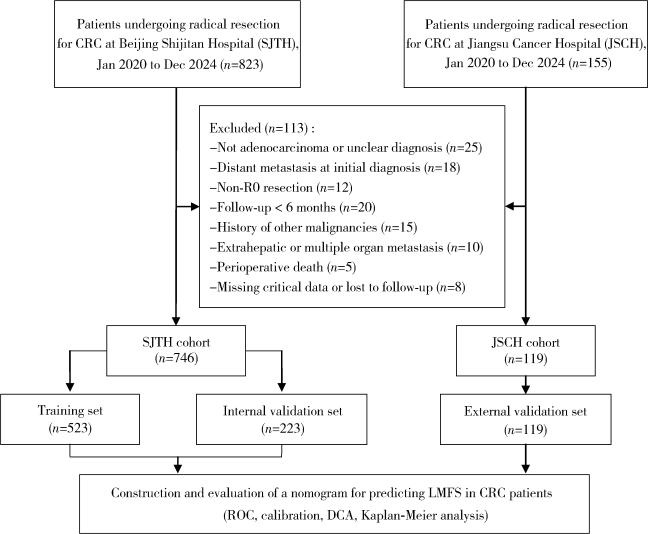
1.2 数据收集
1.3 统计学分析
2 结果
2.1 多中心CRC患者的基线临床病理特征比较
表1 多中心CRC患者的基线临床病理特征比较Table 1 Comparison of baseline clinicopathologic characteristics of CRC patients across multiple centers |
| Variables | SJTH cohort | JSCH cohort | P | ||
| Training set (n=523) | Internal validation set (n=223) | External validation set (n=119) | |||
| Age/years, n (%) | 0.246 | ||||
| < 65 | 298 (57.0) | 138 (61.9) | 77 (64.7) | ||
| ≥65 | 225 (43.0) | 85 (38.1) | 42 (35.3) | ||
| Gender, n (%) | 0.867 | ||||
| Male | 325 (62.1) | 136 (61.0) | 71 (59.7) | ||
| Female | 198 (37.9) | 87 (39.0) | 48 (40.3) | ||
| BMI/(kg/m2), n (%) | 0.115 | ||||
| < 18.5 | 43 (8.2) | 17 (7.6) | 15 (12.6) | ||
| 18.5 - < 24 | 251 (48.0) | 109 (48.9) | 55 (46.2) | ||
| 24 - < 28 | 206 (39.4) | 87 (39.0) | 44 (37.0) | ||
| ≥28 | 23 (4.4) | 10 (4.5) | 5 (4.2) | ||
| CEA/(μg/L), n (%) | 0.372 | ||||
| < 5.0 | 240 (45.9) | 95 (42.6) | 53 (44.5) | ||
| ≥5.0 | 283 (54.1) | 128 (57.4) | 66 (55.5) | ||
| CA199/(U/mL), n (%) | 0.391 | ||||
| < 37 | 245 (46.8) | 97 (43.5) | 47 (39.5) | ||
| ≥37 | 278 (53.2) | 126 (56.5) | 72 (60.5) | ||
| Tumor site, n (%) | 0.092 | ||||
| Ascending colon | 103 (19.7) | 38 (17.0) | 31 (26.1) | ||
| Transverse colon | 13 (2.5) | 13 (5.8) | 4 (3.4) | ||
| Descending colon | 29 (5.5) | 14 (6.3) | 12 (10.1) | ||
| Sigmoid colon | 155 (29.6) | 61 (27.4) | 28 (23.5) | ||
| Rectum | 223 (42.6) | 97 (43.5) | 44 (37.0) | ||
| Differentiation grade, n (%) | 0.238 | ||||
| High | 78 (14.9) | 26 (11.7) | 21 (17.6) | ||
| Moderate | 333 (63.7) | 151 (67.7) | 66 (55.5) | ||
| Low | 112 (21.4) | 46 (20.6) | 32 (26.9) | ||
| Tumor size/cm, n (%) | 0.155 | ||||
| < 5 | 352 (67.3) | 148 (66.3) | 82 (68.9) | ||
| ≥5 | 171 (32.7) | 75 (33.6) | 37 (31.1) | ||
| T stage, n (%) | 0.054 | ||||
| T1 | 47 (9.0) | 18 (8.1) | 6 (5.0) | ||
| T2 | 93 (17.8) | 31 (13.9) | 15 (12.6) | ||
| T3 | 348 (66.5) | 166 (74.4) | 85 (71.4) | ||
| T4 | 35 (6.7) | 8 (3.6) | 13 (10.9) | ||
| N stage, n (%) | 0.875 | ||||
| N0 | 321 (61.4) | 133 (59.6) | 74 (62.2) | ||
| N1 | 128 (24.5) | 58 (26.0) | 32 (26.9) | ||
| N2 | 74 (14.1) | 32 (14.3) | 13 (10.9) | ||
| KRAS, n (%) | 0.779 | ||||
| Mutant type | 256 (48.9) | 112 (50.2) | 55 (46.2) | ||
| Wild type | 267 (51.1) | 111 (49.8) | 64 (53.8) | ||
| NRAS, n (%) | 0.425 | ||||
| Mutant type | 85 (16.3) | 45 (20.2) | 20 (16.8) | ||
| Wild type | 438 (83.7) | 178 (79.8) | 99 (83.2) | ||
| BRAF, n (%) | 0.309 | ||||
| Mutant type | 79 (15.1) | 40 (17.9) | 14 (11.8) | ||
| Wild type | 444 (84.9) | 183 (82.1) | 105 (88.2) | ||
| MSI status, n (%) | 0.287 | ||||
| MSI-H | 110 (21.0) | 49 (22.0) | 18 (15.1) | ||
| MSS | 413 (79.0) | 174 (78.0) | 101 (84.9) | ||
| Vascular invasion, n (%) | 0.296 | ||||
| Yes | 170 (32.5) | 71 (31.8) | 30 (25.2) | ||
| No | 353 (67.5) | 152 (68.2) | 89 (74.8) | ||
| Nerve invasion, n (%) | 0.313 | ||||
| Yes | 174 (33.3) | 71 (31.8) | 31 (26.1) | ||
| No | 349 (66.7) | 152 (68.2) | 88 (73.9) | ||
| Chemotherapy, n (%) | 0.197 | ||||
| Yes | 258 (49.3) | 120 (53.8) | 52 (43.7) | ||
| No | 265 (50.7) | 103 (46.2) | 67 (56.3) | ||
| Targeted therapy, n (%) | 0.112 | ||||
| Yes | 46 (8.8) | 21 (9.4) | 4 (3.4) | ||
| No | 477 (91.2) | 202 (90.6) | 115 (96.6) | ||
CRC, colorectal cancer; SJTH, Beijing Shijitan Hospital; JSCH, Jiangsu Cancer Hospital; BMI,body mass index;CEA,carcinoembryonic antigen;CA199,carbohydrate antigen 19-9;KRAS,kirsten rat sarcoma viral oncogene homolog;NRAS,neuroblastoma RAS viral oncogene homolog;BRAF,b-raf proto-oncogene, serine/threonine kinase;MSI-H,microsatellite instability-high;MSS,microsatellite stability. |
2.2 CRC患者术后肝转移风险因素分析
表2 CRC患者术后无肝转移生存期的Cox回归分析Table 2 Cox regression for liver metastasis-free survival in patients with CRC |
| Variables | Univariate analysis | Multivariate analysis | |||
| P | HR (95%CI) | P | HR (95%CI) | ||
| Age/years | |||||
| < 65 | Reference | Reference | |||
| ≥65 | 0.039 | 1.55 (1.12-1.95) | 0.041 | 1.52 (1.22-1.74) | |
| Gender | |||||
| Female | Reference | ||||
| Male | 0.610 | 1.12 (0.72-1.73) | |||
| BMI/(kg/m2) | |||||
| < 18.5 | Reference | ||||
| 18.5 - < 24 | 0.571 | 1.00 (0.94-1.05) | |||
| 24 - < 28 | 0.173 | 1.23 (0.94-1.45) | |||
| ≥28 | 0.119 | 1.35 (0.95-1.59) | |||
| CEA/(μg/L) | |||||
| < 5.0 | Reference | ||||
| ≥5.0 | 0.422 | 1.19 (0.78-1.82) | |||
| CA199/(U/mL) | |||||
| < 37 | Reference | ||||
| ≥37 | 0.237 | 1.35 (0.82-2.27) | |||
| Tumor site | |||||
| Ascending colon | Reference | ||||
| Transverse colon | 0.352 | 0.38 (0.05-2.90) | |||
| Descending colon | 0.751 | 0.84 (0.27-2.54) | |||
| Sigmoid colon | 0.420 | 1.30 (0.69-2.47) | |||
| Rectum | 0.652 | 1.15 (0.63-2.11) | |||
| Differentiation grade | |||||
| High | Reference | Reference | |||
| Moderate | 0.019 | 1.85 (1.68-2.11) | 0.005 | 1.19 (1.04-1.28) | |
| Low | 0.001 | 2.41 (2.24-2.70) | 0.005 | 2.54 (2.30-2.97) | |
| Tumor size/cm | |||||
| < 5 | Reference | ||||
| ≥5 | 0.119 | 1.26 (0.95-1.54) | |||
| T stage | |||||
| T1 | Reference | Reference | |||
| T2 | 0.005 | 2.89 (1.97-3.42) | 0.038 | 1.59 (1.03-2.38) | |
| T3 | 0.001 | 4.75 (3.55-5.97) | 0.021 | 3.55(2.20-4.68) | |
| T4 | < 0.001 | 8.22 (7.41-10.24) | < 0.001 | 5.21(3.58-6.04) | |
| N stage | |||||
| N0 | Reference | Reference | |||
| N1 | 0.001 | 2.17 (1.69-2.8) | 0.003 | 1.62 (1.18-2.02) | |
| N2 | < 0.001 | 3.96 (2.55-4.80) | < 0.001 | 2.88 (1.96-3.14) | |
| KRAS | |||||
| Wild type | Reference | Reference | |||
| Mutant type | 0.012 | 1.56 (1.35-1.88) | 0.005 | 1.42 (1.27-1.63) | |
| NRAS | |||||
| Wild type | Reference | Reference | |||
| Mutant type | 0.105 | 1.24 (0.89-1.45) | 0.275 | 1.27 (0.93- 1.43) | |
| BRAF | |||||
| Wild type | Reference | Reference | |||
| Mutant type | 0.031 | 1.43 (1.20-1.93) | 0.029 | 1.53 (1.29-1.84) | |
| MSI status | |||||
| MSS | Reference | Reference | |||
| MSI-H | 0.024 | 0.60 (0.47-0.81) | 0.035 | 0.71 (0.54-0.92) | |
| Vascular invasion | |||||
| No | Reference | Reference | |||
| Yes | < 0.001 | 2.78 (1.82-4.25) | 0.017 | 1.90 (1.67-2.28) | |
| Nerve invasion | |||||
| No | Reference | Reference | |||
| Yes | < 0.001 | 2.80 (1.83-4.28) | 0.046 | 1.12 (1.08-1.38) | |
| Chemotherapy | |||||
| No | Reference | Reference | |||
| Yes | < 0.001 | 4.29 (2.55-7.21) | < 0.001 | 2.65 (1.49-4.72) | |
| Targeted therapy | |||||
| No | Reference | Reference | |||
| Yes | < 0.001 | 9.26 (5.16-15.43) | < 0.001 | 8.35 (4.91-14.20) | |
Abbreviations as in Table 1. |
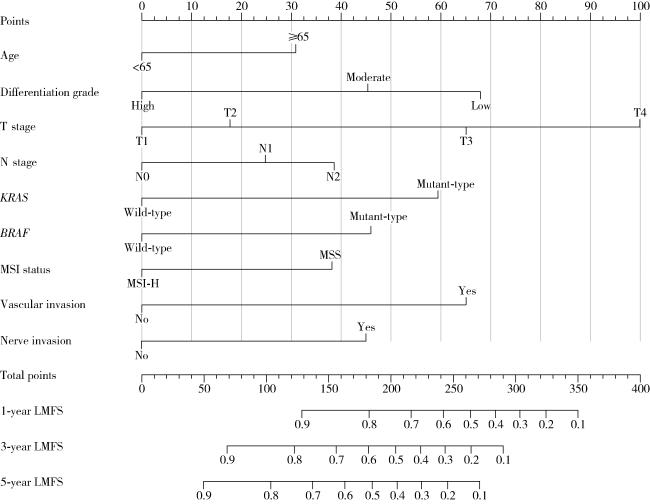
2.3 LMFS列线图预测模型的构建及验证
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
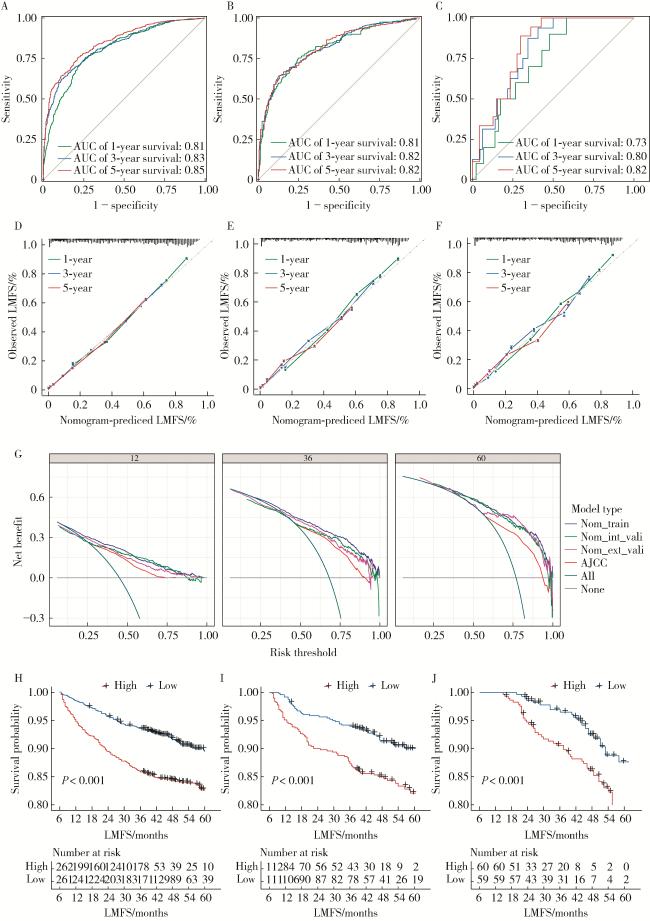
图3 预测CRC患者LMFS列线图模型的综合评估A,B,C,ROC analysis of the nomogram for the LMFS in the training, internal validation, and external validation cohorts;D,E,F,calibration curves of the nomogram for predicting 1-, 3-, and 5-year LMFS in the training, internal validation, and external validation cohorts;G,decision curves of the nomogram for predicting 1-, 3-, and 5-year LMFS;H,I,J,Kaplan-Meier curves of LMFS for patients in the low-and high-risk groups in the training set, internal validation set, and external validation set, respectively. AJCC, American Joint Committee on Cancer. Figure 3 Comprehensive evaluation of the nomogram for predicting liver metastasis-free survival (LMFS) in patients with colorectal cancer (CRC) |
3 讨论
表3 2015—2025年发表的代表性结直肠癌肝转移预测模型特征对比Table 3 Comparison of representative prediction models for colorectal cancer liver metastasis published from 2015 to 2025 |
| Study | Data source | Sample size | Prediction endpoint | Methodology | Variables | Model performance | Validation strategy |
| Yan, et al. (2019)[10] | SEER database | 32 819 | LM & LNM | Logistic regression | Age, CEA, tumor size, grade, N stage | AUC: 0.74-0.81 | Internal random split |
| Li, et al. (2020)[12] | SEER database | 9 958 | OS & CSS | Cox regression | Age, marital status, race, tumor location, pathological grade, histological type, T stage, N stage, colectomy, hepatic surgery, CEA | C-index: 0.749 | Internal validation |
| Hao, et al. (2022)[14] | Single left | 623 | Metachronous LM | Lasso regression | Age, CEA, vascular invasion, T stage, N stage, family history of cancer, KRAS mutation | C-index: 0.787 | Internal validation |
| Xiao, et al. (2022)[15] | Single left | 611 | Metachronous LM | Deep learning (ResNet-50)+Cox | HE image risk score, VELIPI, pT, pN | C-index: 0.807 | Internal validation split (7 ∶3) |
| Shao, et al. (2024)[16] | SEER database | 4 981 | OS & CSS | Cox & competing risk models | Age, race, grade, T stage, N stage, surgery, chemotherapy, CEA, tumor deposits, lung metastasis, tumor size | C-index: 0.74- 0.79 | Internal random split (7 ∶3) |
| Jing, et al. (2025)[17] | Single left | 212 | Postoperative liver metastasis | Random forest (fusion model) | CT radiomics features + Clinical data | AUC: 0.751 | Internal random split |
SEER, Surveillance, Epidemiology, and End Results; OS,overall survival;CSS,cancer-specific survival;LM,liver metastasis;LNM,lymph node metastasis; CEA, carcinoembryonic antigen. |