
1 资料与方法
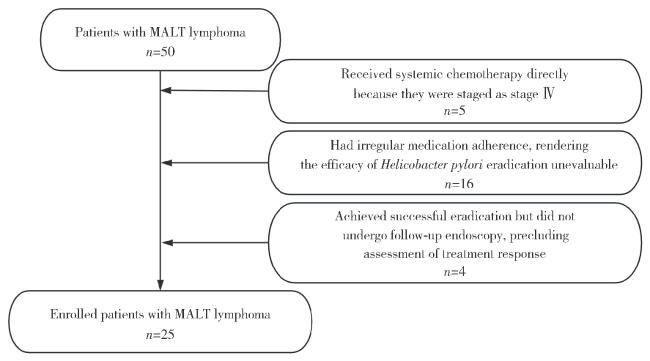
1.1 病例选择
1.2 研究方法
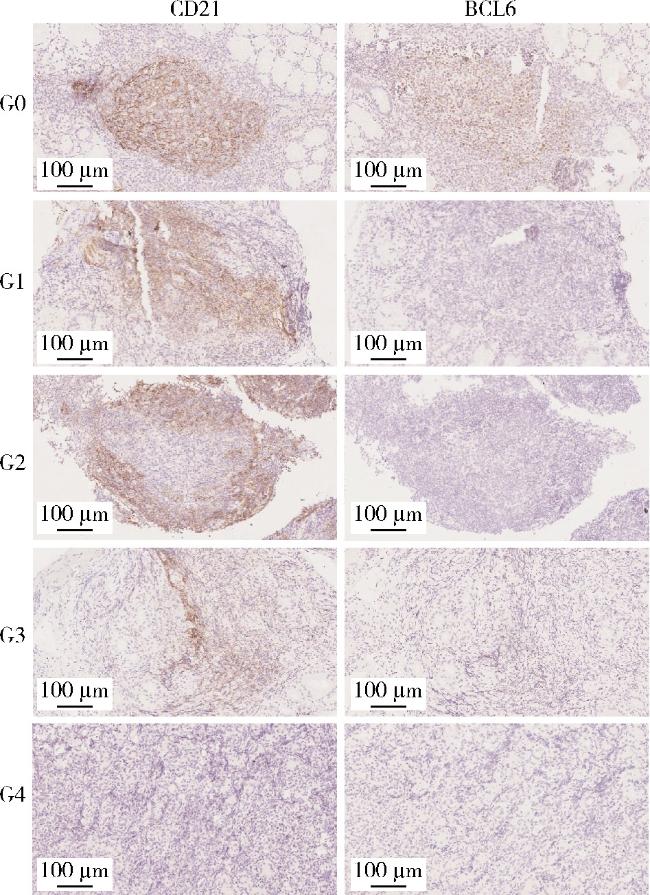
表1 淋巴滤泡破坏程度分级Table 1 Grading of lymphoid follicular architecture disruption |
| Grade | Name | Histomorphological features |
| G0 | Architecture-intact type | A continuous, dense CD21 meshwork surrounds a well-defined BCL6-positive germinal center; The follicular contour is intact, with no disruption |
| G1 | Marginal thinning/eccentric type | The CD21 meshwork remains continuous but shows peripheral “crescent-shaped” condensation toward the outer margin or focal thinning; The germinal center remains intact |
| G2 | Disrupted with preserved outline type | The CD21 meshwork shows breaks and/or gaps; The follicular outline is still preserved. Features suggestive of tumor cell “follicular colonization” are present (BCL6-positive areas are intercalated by non-germinal-center cells) |
| G3 | Outline-loss type | The follicular contour is indistinct or largely lost; Only scattered fragmentary CD21 meshwork persists, and BCL6-positive germinal-center cells are no longer detectable |
| G4 | Absent/disintegrated type | The CD21 meshwork is almost completely unrecognizable/absent; Germinal centers are lost, or only rare scattered BCL6-positive cells are seen |
CD21, complement receptor type 2; BCL6, B-cell lymphoma 6 protein. |
1.3 统计学分析
2 结果
2.1 基本信息
2.2 基线资料
表2 100例PGL患者的基线资料Table 2 Baseline data of 100 primary gastric lymphma (PGL) patients |
| Indicator | Indolent lymphoma (n=51) | Aggressive lymphoma (n=49) | P |
| Gender | 0.680 | ||
| Male | 25 (49.0) | 22 (44.9) | |
| Female | 26 (51.0) | 27 (55.1) | |
| Age/years | |||
| Male | 63.52±8.71a | 60.68±14.34a | 0.410 |
| Female | 59.88±12.90a | 65.26±11.84a | 0.120 |
| Presenting symptoms | 0.137 | ||
| Abdominal pain | 13 (25.5) | 22 (44.9) | |
| Abdominal distension | 8 (15.7) | 5 (10.2) | |
| Acid reflux/heartburn | 3 (5.9) | 3 (6.1) | |
| Nausea/vomiting | 4 (7.8) | 4 (8.2) | |
| Hematemesis/melena | 8 (15.7) | 10 (20.4) | |
| Asymptomatic | 15 (29.4) | 5 (10.2) | |
| Hypertension | 0.790 | ||
| No | 32 (62.7) | 32 (65.3) | |
| Yes | 19 (37.3) | 17 (34.7) | |
| Diabetes mellitus | 0.716 | ||
| No | 44 (86.3) | 41 (83.7) | |
| Yes | 7 (13.7) | 8 (16.3) | |
| Smoking | 0.722 | ||
| No | 38 (74.5) | 38 (77.6) | |
| Yes | 13 (25.5) | 11 (22.4) | |
| Alcohol consumption | 0.315 | ||
| No | 41 (80.4) | 43 (87.8) | |
| Yes | 10 (19.6) | 6 (12.2) | |
| B symptoms | 0.004 | ||
| No | 40 (80.4) | 25 (51.0) | |
| Yes | 11 (19.6) | 24 (49.0) |
Data are n(%) or ${\bar x}$±s. a,normality was assessed using the Shapiro-Wilk test, and the data were consistent with a normal distribution. |
2.3 内镜资料
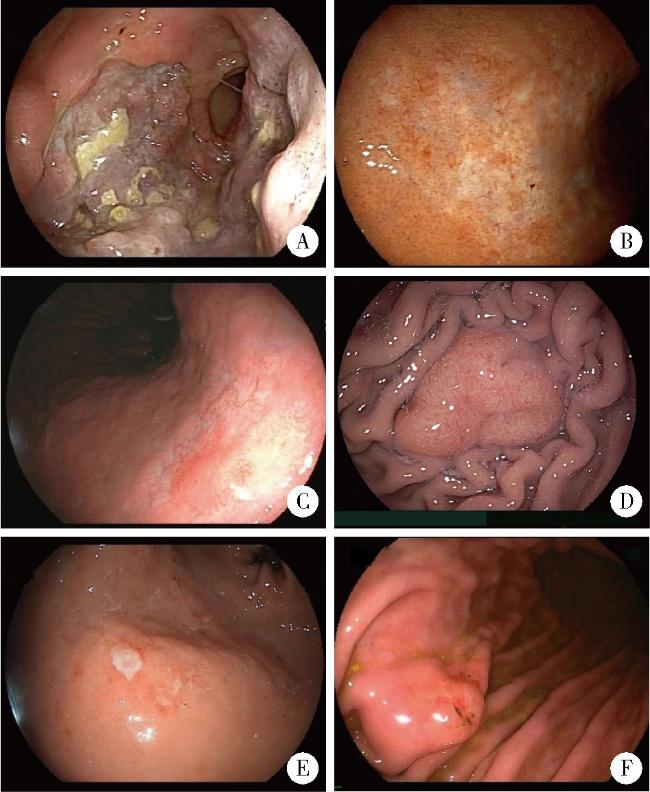
表3 100例PGL患者的内镜结果Table 3 Endoscopic characteristics of 100 PGL patients |
| Indicator | Indolent lymphoma (n=51) | Aggressive lymphoma (n=49) | P |
| Lesion locationb | 0.104 | ||
| Cardia | 0 (0.0) | 1 (1.2) | |
| Fundus | 7 (8.8) | 5 (6.0) | |
| Upper gastric body | 18 (22.5) | 9 (10.8) | |
| Middle gastric body | 22 (27.5) | 19 (22.9) | |
| Lower gastric body | 22 (27.5) | 27 (32.5) | |
| Antrum | 11 (13.7) | 22 (26.6) | |
| Lesion orientation | 0.103 | ||
| Anterior wall | 13 (25.5) | 8 (16.3) | |
| Posterior wall | 6 (11.8) | 9 (18.4) | |
| Lesser curvature | 7 (13.7) | 15 (30.6) | |
| Greater curvature | 25 (49.0) | 17 (34.7) | |
| Gross morphology | < 0.001 | ||
| Ulcerative type | 11 (21.6) | 35 (71.4) | |
| Infiltrative type | 12 (23.5) | 0 (0.0) | |
| Nodular type | 19 (37.3) | 1 (2.0) | |
| Polypoid type | 4 (7.8) | 1 (2.0) | |
| Mixed type | 5 (9.8) | 12 (24.6) | |
| Number of lesions | 0.568 | ||
| Solitary | 19 (37.3) | 21 (42.9) | |
| Multiple | 32 (62.7) | 28 (57.1) | |
| Long diameter/cmc | 0.178a | ||
| <1 | 7 (23.3) | 4 (12.9) | |
| 1-<3 | 16 (53.4) | 13 (41.9) | |
| ≥3 | 7 (23.3) | 14 (45.2) | |
| Short diameter/cmc | 0.131a | ||
| <1 | 11 (36.7) | 8 (25.8) | |
| 1-<3 | 15 (50.0) | 12 (38.7) | |
| ≥3 | 4 (13.3) | 11 (35.5) | |
| Erosion | < 0.001 | ||
| Absent | 26 (51.0) | 1 (2.0) | |
| Present | 25 (49.0) | 48 (98.0) | |
| Ulceration/white slough | < 0.001 | ||
| Absent | 32 (62.7) | 2 (4.0) | |
| Present | 19 (37.3) | 47 (96.0) | |
| Consistency | < 0.001 | ||
| Soft | 32 (62.7) | 8 (16.3) | |
| Hard | 4 (7.8) | 5 (10.2) | |
| Tough/firm | 9 (17.6) | 13 (26.5) | |
| Brittle | 6 (11.9) | 23 (47.0) | |
| Bleeding | 0.008 | ||
| Active bleeding | 4 (7.8) | 9 (18.4) | |
| Easy bleeding on biopsy | 40 (78.4) | 40 (81.6) | |
| Not prone to bleeding | 7 (13.8) | 0 (0.0) | |
| Perilesional mucosa | 0.550 | ||
| Normal mucosa | 1 (2.0) | 0 (0.0) | |
| Erythema/edema | 21 (41.2) | 16 (32.7) | |
| Converging folds | 6 (11.8) | 5 (10.2) | |
| Uneven mucosa | 23 (45.0) | 28 (57.1) | |
| Background mucosa | 0.259 | ||
| Normal mucosa | 4 (7.8) | 2 (4.1) | |
| Erythema/edema | 5 (9.8) | 5 (10.2) | |
| Mottled mucosa | 32 (62.7) | 24 (49.0) | |
| Uneven mucosa | 10 (19.7) | 18 (36.7) | |
| Gastric lumen | < 0.001 | ||
| Patent | 51 (100.0) | 30 (61.2) | |
| Stenosis | 0 (0.0) | 19 (38.8) | |
| Peristalsis | < 0.001 | ||
| Good | 46 (90.2) | 25 (51.0) | |
| Poor | 5 (9.8) | 24 (49.0) |
Data are n(%). a, ordinal variables were analyzed using the Wilcoxon rank-sum test; b, classified according to the primary lesion location; c, data were missing for 21 patients in the indolent lymphoma group and 18 patients in the aggressive lymphoma group; PGL, primary gastric lymphma. |
2.4 分期/治疗资料
表4 100例PGL患者的分期/治疗资料Table 4 Staging and treatment data of 100 PGL patients |
| Indicator | Indolent lymphoma (n=51) | Aggressive lymphoma (n=49) | P |
| Lugano classification | < 0.001a | ||
| Stage Ⅰ | 37 (72.5) | 8 (16.3) | |
| Stage Ⅱ | 9 (17.6) | 9 (18.4) | |
| Stage Ⅲ | 0 (0.0) | 2 (4.1) | |
| Stage Ⅳ | 5 (9.9) | 30 (61.2) | |
| Therapeutic regimen | < 0.001 | ||
| Untreated | 6 (11.8) | 4 (8.2) | |
| HPE only | 16 (31.4) | 0 (0.0) | |
| Radiotherapy/chemotherapy/surgery | 7 (13.7) | 42 (85.7) | |
| HPE+Radiotherapy/chemotherapy | 22 (43.1) | 3 (6.1) | |
| Follow-up effect | 0.007 | ||
| Remission after treatment | 31 (60.7) | 30 (61.2) | |
| Residual/ineffective | 8 (15.7) | 1 (2.0) | |
| Progress/death | 6 (11.8) | 16 (32.7) | |
| Untreated and alive | 6 (11.8) | 2 (4.1) |
Data are n(%). a,ordinal variables were analyzed using the Wilcoxon rank-sum test; PGL, primary gastric lymphma. |
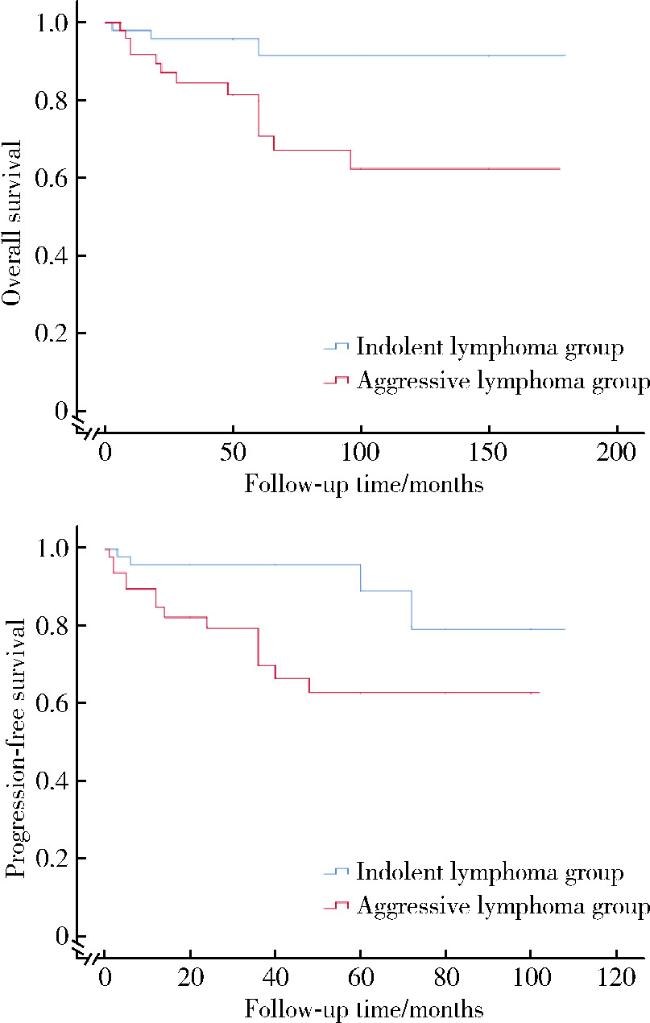
2.5 生存资料
2.6 淋巴滤泡破坏程度分级
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
2.7 危险因素分析
表5 根除有效组和根除无效组的组间比较Table 5 Inter group comparison of HPE effective group and HPE ineffective group |
| Indicator | HPE effective (n=10) | HPE ineffective (n=15) | P |
| Gender | 0.099 | ||
| Male | 2 (20.0) | 9 (60.0) | |
| Female | 8 (80.0) | 6 (40.0) | |
| Age/years | 61.1 (52.8, 68.0) | 62.9 (59.0, 69.0) | 0.453 |
| Hypertension | >0.999 | ||
| No | 6 (60.0) | 9 (60.0) | |
| Yes | 4 (40.0) | 6 (40.0) | |
| Diabetes mellitus | >0.999 | ||
| No | 8 (80.0) | 13 (86.7) | |
| Yes | 2 (20.0) | 2 (13.3) | |
| Smoking | 0.179 | ||
| No | 9 (90.0) | 9 (60.0) | |
| Yes | 1 (10.0) | 6 (40.0) | |
| Alcohol | 0.615 | ||
| No | 9 (90.0) | 11 (73.3) | |
| Yes | 1 (10.0) | 4 (26.7) | |
| B symptoms | 0.499 | ||
| No | 7 (70.0) | 13 (86.7) | |
| Yes | 3 (30.0) | 2 (13.3) | |
| Lesion orientation | >0.999 | ||
| Anterior wall | 2 (20.0) | 2 (13.3) | |
| Posterior wall | 1 (10.0) | 1 (6.7) | |
| Lesser curvature | 2 (20.0) | 3 (20.0) | |
| Greater curvature | 5 (50.0) | 9 (60.0) | |
| Gross morphology | 0.912 | ||
| Ulcerative type | 1 (10.0) | 2 (13.3) | |
| Infiltrative type | 2 (20.0) | 2 (13.3) | |
| Nodular type | 6 (60.0) | 8 (53.5) | |
| Polypoid type | 0 (0.0) | 2 (13.3) | |
| Mixed type | 1 (10.0) | 1 (6.7) | |
| Number of lesions | >0.999 | ||
| Solitary | 3 (30.0) | 5 (33.3) | |
| Multiple | 7 (70.0) | 10 (66.7) | |
| Erosion | >0.999 | ||
| Absent | 6 (60.0) | 9 (60.0) | |
| Present | 4 (40.0) | 6 (40.0) | |
| Ulceration | >0.999 | ||
| Absent | 7 (70.0) | 11 (73.3) | |
| Present | 3 (30.0) | 4 (26.7) | |
| Consistency | 0.510 | ||
| Soft | 5 (50.0) | 11 (73.3) | |
| Hard | 1 (10.0) | 0 (0.0) | |
| Tough | 1 (10.0) | 2 (13.3) | |
| Brittle | 3 (30.0) | 2 (13.3) | |
| Peristalsis | 0.400 | ||
| Good | 9 (90.0) | 15 (100.0) | |
| Poor | 1 (10.0) | 0 (0.0) | |
| Hp infection status | 0.049 | ||
| Positive | 7 (70.0) | 4 (26.7) | |
| Negative | 3 (30.0) | 11 (73.3) | |
| Disruption grading | 0.015 | ||
| G0 | 3 (30.0) | 0 (0.0) | |
| G1 | 1 (10.0) | 0 (0.0) | |
| G2 | 4 (40.0) | 3 (20.0) | |
| G3 | 0 (0.0) | 8 (53.3) | |
| G4 | 2 (20.0) | 4 (26.7) |
Data are n(%) or M (P25, P75). Not all variables were normally distributed in both groups. |