Journal of Peking University (Health Sciences) ›› 2024, Vol. 56 ›› Issue (5): 874-883. doi: 10.19723/j.issn.1671-167X.2024.05.019
Previous Articles Next Articles
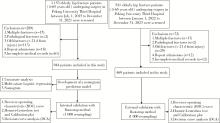
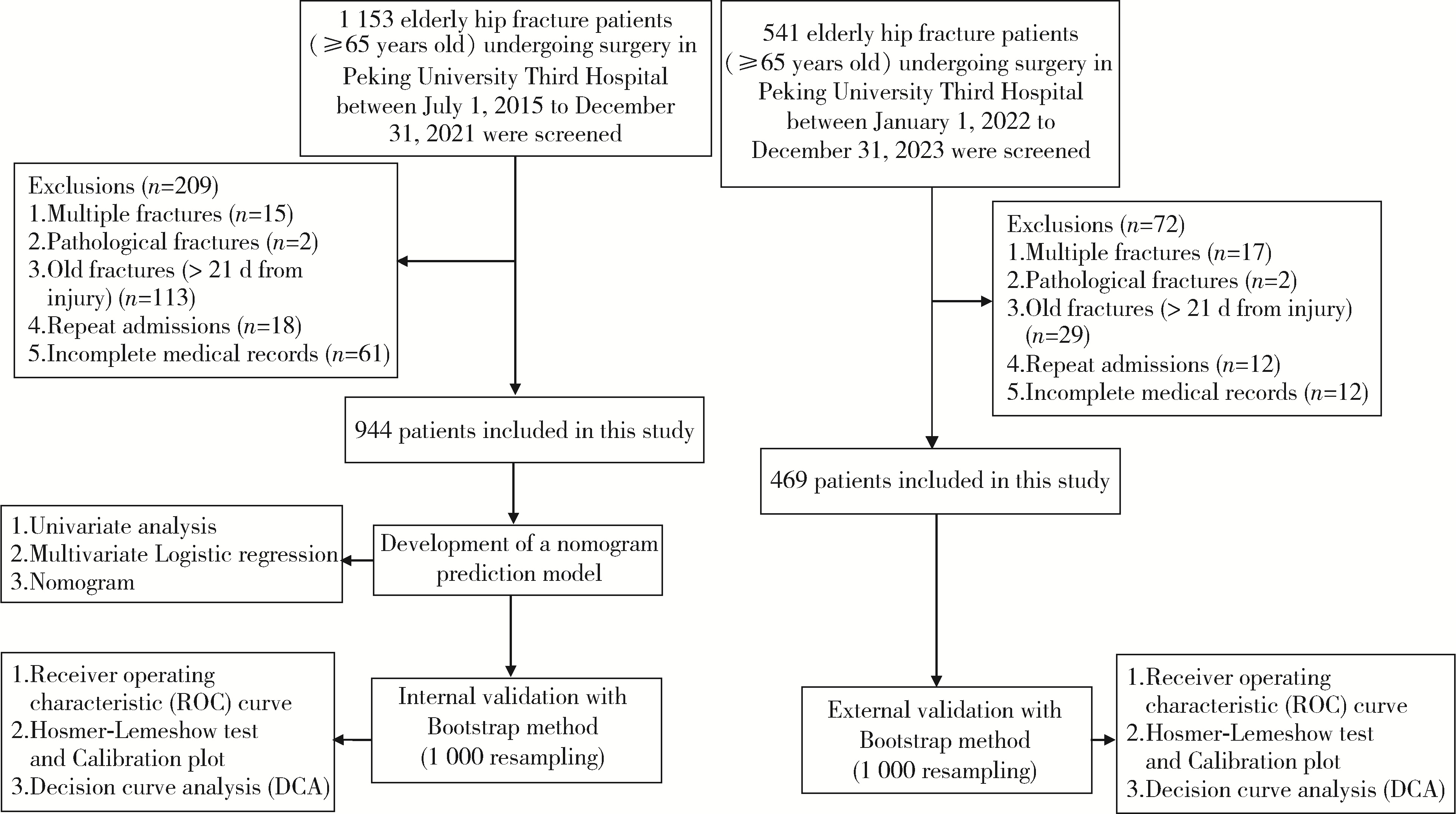
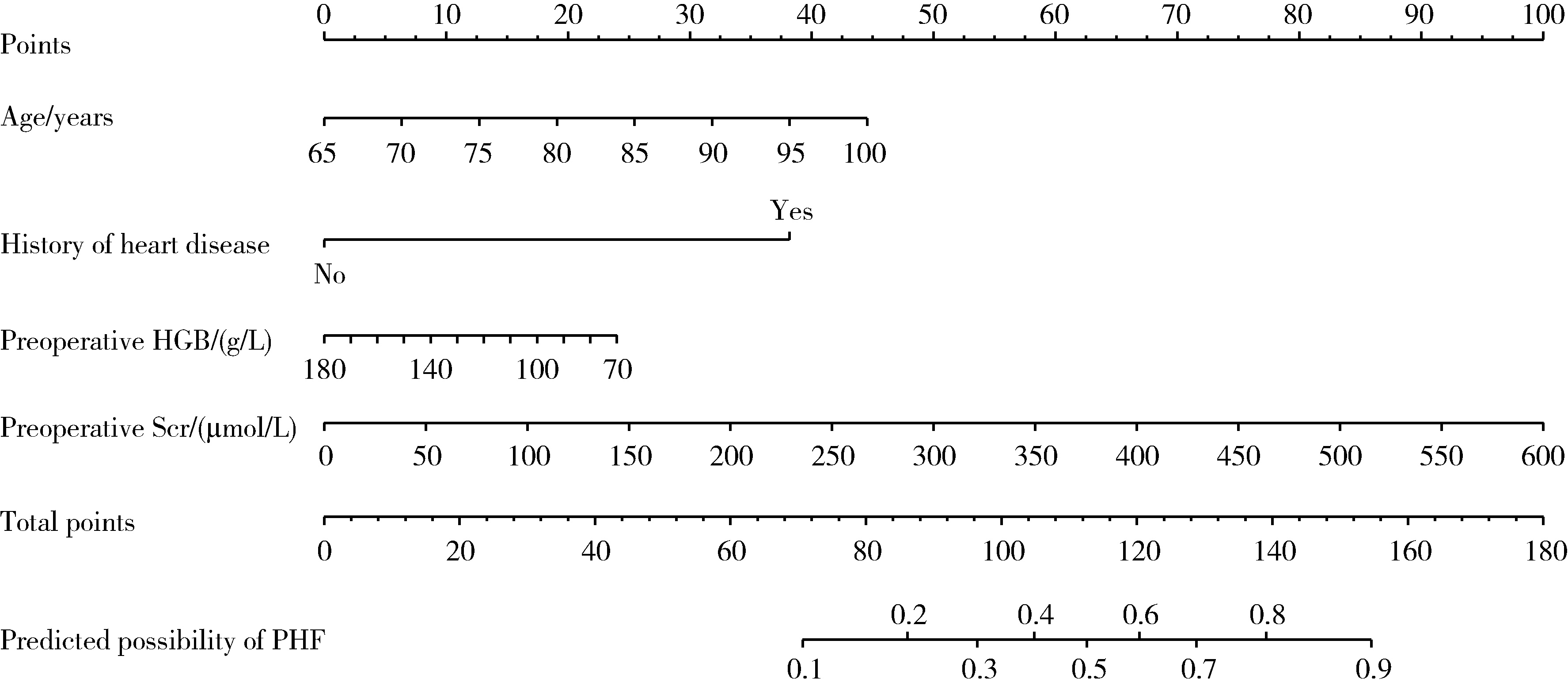
Construction and validation of a nomogram for predicting in-hospital postoperative heart failure in elderly patients with hip fracture
Yuanmei LIU, Yicheng FU, Jingxin HAO, Fuchun ZHANG, Huilin LIU*( )
)
- Department of Geriatrics, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R541.6



| 1 |
Roche JJ , Wenn RT , Sahota O , et al. Effect of comorbidities and postoperative complications on mortality after hip fracture in elderly people: Prospective observational cohort study[J]. BMJ, 2005, 331 (7529): 1374.
doi: 10.1136/bmj.38643.663843.55 |
| 2 |
Cullen MW , Gullerud RE , Larson DR , et al. Impact of heart failure on hip fracture outcomes: A population-based study[J]. J Hosp Med, 2011, 6 (9): 507- 512.
doi: 10.1002/jhm.918 |
| 3 | Cordero J , Maldonado A , Iborra S . Surgical delay as a risk factor for wound infection after a hip fracture[J]. Injury, 2016, 47 (Suppl 3): S56- S60. |
| 4 |
You F , Ma C , Sun F , et al. The risk factors of heart failure in elderly patients with hip fracture: What should we care?[J]. BMC Musculoskelet Disord, 2021, 22 (1): 832.
doi: 10.1186/s12891-021-04686-8 |
| 5 |
Tian M , Li W , Wang Y , et al. Risk factors for perioperative acute heart failure in older hip fracture patients and establishment of a nomogram predictive model[J]. J Orthop Surg Res, 2023, 18 (1): 347.
doi: 10.1186/s13018-023-03825-2 |
| 6 |
Brown CA , Boling J , Manson M , et al. Relation between prefracture characteristics and perioperative complications in the elderly adult patient with hip fracture[J]. South Med J, 2012, 105 (6): 306- 310.
doi: 10.1097/SMJ.0b013e3182574bfd |
| 7 |
季日旭, 陈作喜, 吴银生, 等. 老年股骨颈骨折关节置换围术期发生心功能衰竭的危险因素分析[J]. 中华创伤杂志, 2018, 34 (11): 1030- 1034.
doi: 10.3760/cma.j.issn.1001-8050.2018.11.014 |
| 8 |
李长华, 王伟良, 林光锚, 等. 老年股骨转子间骨折患者围手术期发生心力衰竭的相关因素分析[J]. 中华创伤骨科杂志, 2018, 20 (5): 407- 411.
doi: 10.3760/cma.j.issn.1671-7600.2018.05.007 |
| 9 | 梅迎晨, 韩蕊, 陈游洲, 等. 老年髋部骨折围术期心力衰竭的临床特点及危险因素分析[J]. 中国医刊, 2021, 56 (2): 140- 144. |
| 10 |
Gualandro DM , Puelacher C , Chew MS , et al. Acute heart failure after non-cardiac surgery: Incidence, phenotypes, determinants and outcomes[J]. Eur J Heart Fail, 2023, 25 (3): 347- 357.
doi: 10.1002/ejhf.2773 |
| 11 |
McDonagh TA , Metra M , Adamo M , et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure[J]. Eur Heart J, 2021, 42 (36): 3599- 3726.
doi: 10.1093/eurheartj/ehab368 |
| 12 |
Collins GS , Reitsma JB , Altman DG , et al. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement[J]. Ann Intern Med, 2015, 162 (1): 55- 63.
doi: 10.7326/M14-0697 |
| 13 |
Hao G , Wang X , Chen Z , et al. Prevalence of heart failure and left ventricular dysfunction in China: The China Hypertension Survey, 2012-2015[J]. Eur J Heart Fail, 2019, 21 (11): 1329- 1337.
doi: 10.1002/ejhf.1629 |
| 14 |
Jiang Y , Luo Y , Li J , et al. Chronic kidney disease and risk of postoperative cardiovascular events in elderly patients receiving hip fracture surgery[J]. Injury, 2022, 53 (2): 596- 602.
doi: 10.1016/j.injury.2021.12.032 |
| 15 |
Liu Y , Liu H , Zhang F . Development and internal validation of a nomogram for predicting postoperative cardiac events in elderly hip fracture patients[J]. Clin Interv Aging, 2023, 18, 2063- 2078.
doi: 10.2147/CIA.S435264 |
| 16 |
Ye CY , Liu A , Xu MY , et al. Arthroplasty versus internal fixation for displaced intracapsular femoral neck fracture in the elderly: Systematic review and meta-analysis of short- and long-term effectiveness[J]. Chin Med J (Engl), 2016, 129 (21): 2630- 2638.
doi: 10.4103/0366-6999.192788 |
| 17 |
Fisher MA , Matthei JD , Obirieze A , et al. Open reduction internal fixation versus hemiarthroplasty versus total hip arthroplasty in the elderly: A review of the National Surgical Quality Improvement Program database[J]. J Surg Res, 2013, 181 (2): 193- 198.
doi: 10.1016/j.jss.2012.07.004 |
| 18 |
Miller AG , Bercik MJ , Ong A . Nonagenarian hip fracture: Treatment and complications[J]. J Trauma Acute Care Surg, 2012, 72 (5): 1411- 1415.
doi: 10.1097/TA.0b013e318246f3f8 |
| 19 |
O'Hara DA , Duff A , Berlin JA , et al. The effect of anesthetic technique on postoperative outcomes in hip fracture repair[J]. Anesthesiology, 2000, 92 (4): 947- 957.
doi: 10.1097/00000542-200004000-00011 |
| 20 |
Chen X , Li H , Li S , et al. Comparison of risk of complication between neuraxial anaesthesia and general anaesthesia for hip fracture surgery: A systematic review and meta-analysis[J]. Int J Surg, 2023, 109 (3): 458- 468.
doi: 10.1097/JS9.0000000000000291 |
| 21 |
Weinstein ER , Boyer RB , White RS , et al. Improved outcomes for spinal versus general anesthesia for hip fracture surgery: A retrospective cohort study of the National Surgical Quality Improvement Program[J]. Reg Anesth Pain Med, 2024, 49 (1): 4- 9.
doi: 10.1136/rapm-2022-104217 |
| 22 |
Chowdary AR , Beale J , Martinez J , et al. Postoperative complications of spinal vs general anesthesia in elderly patients undergoing hip hemiarthroplasty[J]. Arch Orthop Trauma Surg, 2023, 143 (9): 5615- 5621.
doi: 10.1007/s00402-023-04876-0 |
| [1] | Zhicun LI, Tianyu WU, Lei LIANG, Yu FAN, Yisen MENG, Qian ZHANG. Risk factors analysis and nomogram model construction of postoperative pathological upgrade of prostate cancer patients with single core positive biopsy [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 896-901. |
| [2] | Zezhen ZHOU,Shaohui DENG,Ye YAN,Fan ZHANG,Yichang HAO,Liyuan GE,Hongxian ZHANG,Guoliang WANG,Shudong ZHANG. Predicting the 3-year tumor-specific survival in patients with T3a non-metastatic renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 673-679. |
| [3] | LIU Jie,GUO Chao. A prospective cohort study of the influence of positive/negative effectivity on the mortality risk of the Chinese elderly [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 255-260. |
| [4] | Ming-xin AO,Xue-min LI,Yuan-yuan YU,Hui-juan SHI,Hong-shi HUANG,Ying-fang AO,Wei WANG. Effects of visual restoration on dynamic plantar pressure features in elder individuals [J]. Journal of Peking University (Health Sciences), 2021, 53(5): 907-914. |
| [5] | Wei ZHANG,Pei-xun ZHANG. Analysis of prophylactic effect of extended-duration anticoagulant drugs in elderly patients undergoing hip fracture [J]. Journal of Peking University(Health Sciences), 2019, 51(3): 501-504. |
| [6] | Yi-ran ZHANG,Feng RAO,Wei PI,Pei-xun ZHANG,Bao-guo JIANG. Proximal femoral nails antirotation and dynamic hip screws for fixation of unstable intertrochanteric fractures of femur: A meta-analysis [J]. Journal of Peking University(Health Sciences), 2019, 51(3): 493-500. |
| [7] | Jian CHEN,Cai-hong ZUO,Cai-yi ZHANG,Ming YANG,Pei-xun ZHANG. Comparison of the effects of two cephalomedullary nails (zimmer natural nail and proximal femoral nail antirotation) in treatment of elderly intertrochan teric fractures [J]. Journal of Peking University(Health Sciences), 2019, 51(2): 283-287. |
| [8] | LIU Yu-qing, LU Jian, HAO Yi-chang, XIAO Chun-lei, MA Lu-lin. Predicting model based on risk factors for urosepsis after percutaneous nephrolithotomy [J]. Journal of Peking University(Health Sciences), 2018, 50(3): 507-513. |
| [9] | WEI Bin, ZHANG Hua, XU Mao, LI Min, WANG Jun, ZHANG Li-ping, GUO Xiang-yang, ZHAO Yi-ming, ZHOU Fang. Effect of different anesthetic methods on postoperative outcomes in elderly patients undergoing hip fracture surgery [J]. Journal of Peking University(Health Sciences), 2017, 49(6): 1008-1013. |
| [10] | LI Hao, ZHANG You-Yi. Roles of proinflammatory cytokines in cardiac remodeling induced by sympathetic nervous system /catecholamine [J]. Journal of Peking University(Health Sciences), 2014, 46(6): 1001-1004. |
|
||