Journal of Peking University(Health Sciences) ›› 2019, Vol. 51 ›› Issue (4): 641-645. doi: 10.19723/j.issn.1671-167X.2019.04.008
Previous Articles Next Articles
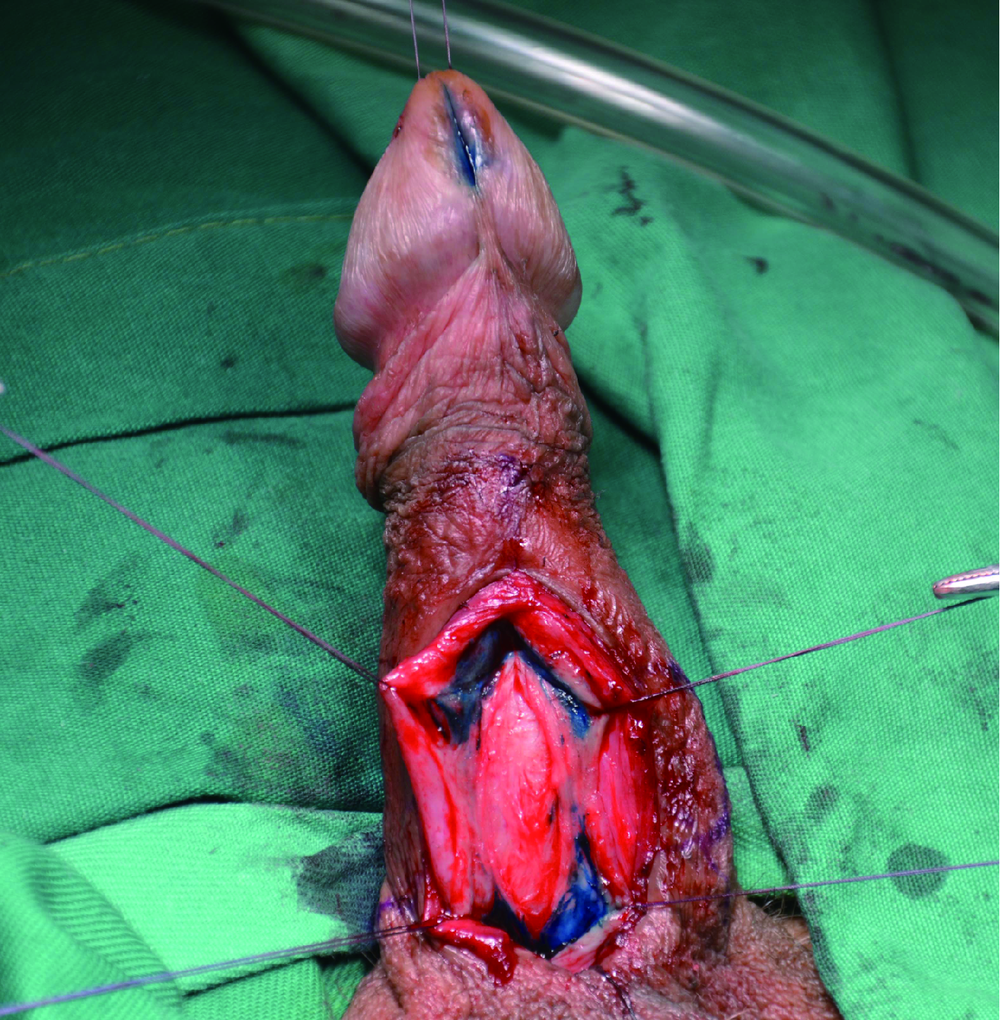
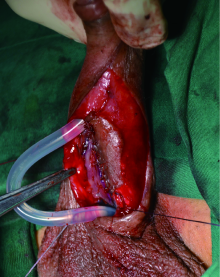
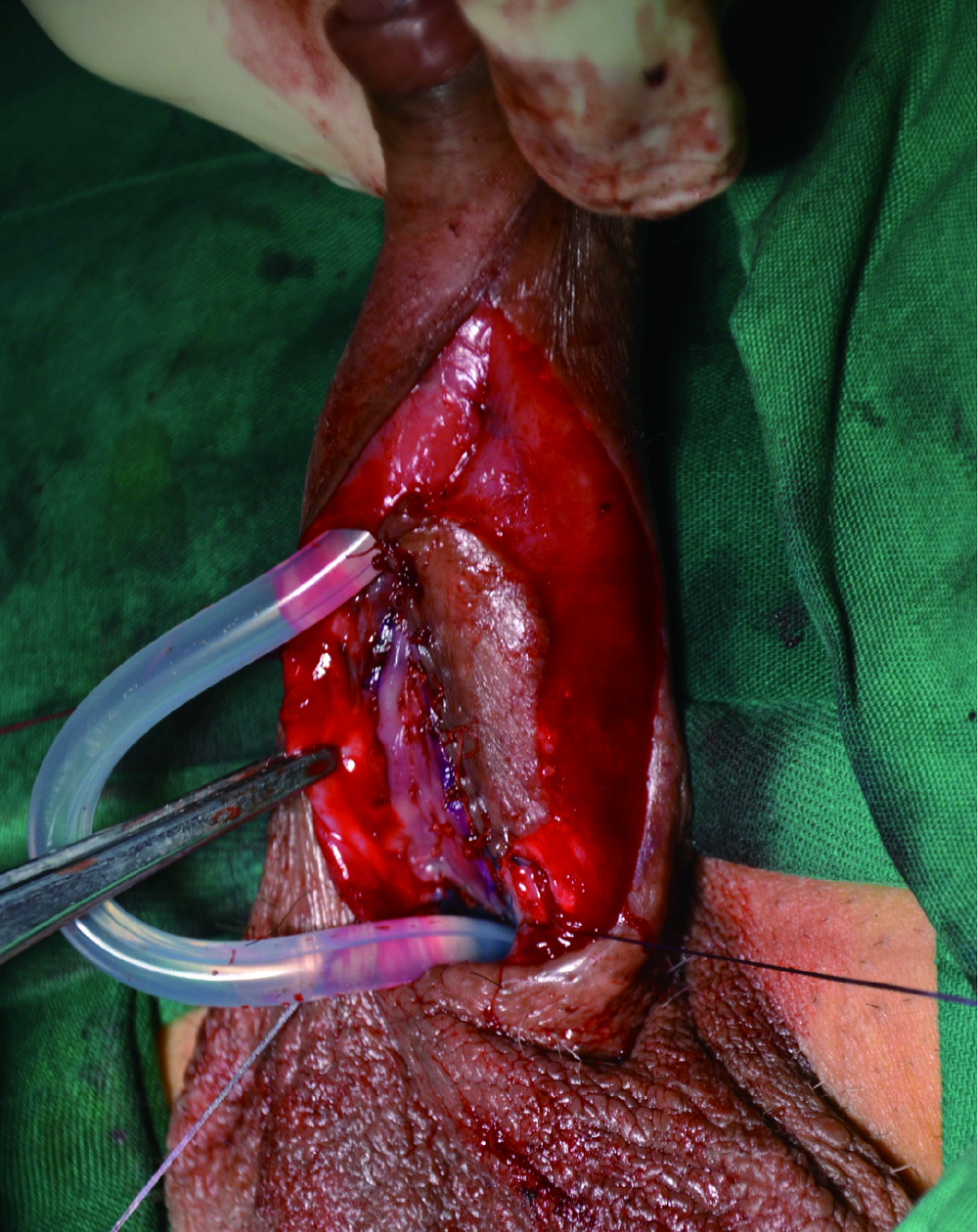
Single-stage repair of penile urethral stricture using combined dorsal onlay oral mucosa grafting with ventral onlay penile skin flap
Jian-wei WANG,Li-bo MAN( ),Guang-lin HUANG,Feng HE,Hai WANG,Hai-dong WANG,Xiao XU,Wei LI,Jian-po ZHAI,Zhen-hua LIU
),Guang-lin HUANG,Feng HE,Hai WANG,Hai-dong WANG,Xiao XU,Wei LI,Jian-po ZHAI,Zhen-hua LIU
- Department of Urology, Beijing Jishuitan Hospital, The Fourth Medical College of Peking University, Beijing 100096, China
CLC Number:
- R699









| [1] | McAninch JW, Morey AF . Penile circular fasciocutaneous skin flap in 1-stage reconstruction of complex anterior urethral strictures[J]. J Urol, 1998,159(4):1209-1213. |
| [2] | Morey AF . Urethral plate salvage with dorsal graft promotes successful penile flaponlay reconstruction of severe pendulous strictures[J]. J Urol, 2001,166(4):1376-1378. |
| [3] | Bayne DB, Gaither TW, Awad MA , et al. Guidelines of guidelines: a review of urethral stricture evaluation, management, and follow-up[J]. Transl Androl Urol, 2017,6(2):288-294. |
| [4] | Horiguchi A . Substitution urethroplasty using oral mucosa graft for male anterior urethral stricture disease: current topics and reviews[J]. Int J Urol, 2017,24(7):493-503. |
| [5] | Erickson BA, Breyer BN , McAninch JW. Single-stage segmental urethral replacement using combined ventral onlay fasciocutaneous flap with dorsal onlay buccal grafting for long segment strictures[J]. BJU Int, 2012,109(9):1392-1396. |
| [6] | Greenwell TJ, Venn AF, Mundy AR . Changing practice in anteriorurethroplasty[J]. BJU Int, 1999,83(6):631-635. |
| [7] | Wessells H, Angermeier KW, Elliott S , et al. Male urethral stricture: American Urological Association Guideline[J]. J Urol, 2017,197(1):182-190. |
| [8] | Gelman J, Sohn W . 1-stage repair of obliterative distal urethral strictures with buccal graft urethral plate reconstruction and simultaneous onlay penile skin flap[J]. J Urol, 2011,186(3):935-938. |
| [9] | Djordjevic ML, Majstorovic M, Stanojevic D , et al. Combined buccal mucosa graft and dorsal penile skin flap for repair of severe hypospadias[J]. Urology, 2008,71(5):821-825. |
| [10] | Soliman MG, Abo Farha MA, El Abd AS , et al. Dorsal onlay urethroplasty using buccal mucosa graft versus penile skin flap for management of long anterior urethral strictures: a prospective randomized study[J]. Scand J Urol, 2014,48(5):466-473. |
| [11] | 满立波, 王建伟 . 图解尿道成形术[M]. 北京: 人民卫生出版社, 2018: 52-59. |
| [1] | Wenyuan LENG, Duan GAO, Xiaoyu LI, Wei ZUO, Weimin HU, Zhenpeng ZHU, Chunru XU, Jian LIN, Xuesong LI. Comparison of efficacy and safety of oral mucosa grafts and acellular dermal matrix grafts in the treatment of long-segment urethral stricture [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 975-979. |
| [2] | Jie WANG, Jianwei WANG, Haizhui XIA, Xiao XU, Jianpo ZHAI, Feng HE, Guanglin HUANG, Guizhong LI. Surgical management of the distal urethral stricture diseases [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1075-1082. |
| [3] | WANG Jian-wei,XU Xiao,BAO Zheng-qing,LIU Zhen-hua,HE Feng,HUANG Guang-lin,MAN Li-bo. Outcomes of partial pubectomy assisted anastomotic urethroplasty for male patients with pelvic fracture urethral distraction defect [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 798-802. |
| [4] | Jian-wei WANG,Li-bo MAN,Xiao XU,Zhen-hua LIU,Feng HE,Guang-lin HUANG,Jian-po ZHAI,Ning ZHOU,Wei LI. Combined transperineal and transpubic urethroplasty for patients with complex male pelvic fracture urethral distraction defect [J]. Journal of Peking University (Health Sciences), 2020, 52(4): 646-650. |
| [5] | WANG Jian-wei, MAN Li-bo, HUANG Guang-lin, WANG Hai, Xu Xiao, ZHU Xiao-fei, LI Wei, LIU Zhen-hua. “3-step” strategy of transperineal anastomotic urethroplasty for the simple pelvic fracture urethral distraction defect in male patients [J]. Journal of Peking University(Health Sciences), 2018, 50(4): 617-620. |
|
||