Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (3): 573-579. doi: 10.19723/j.issn.1671-167X.2021.03.022
Previous Articles Next Articles
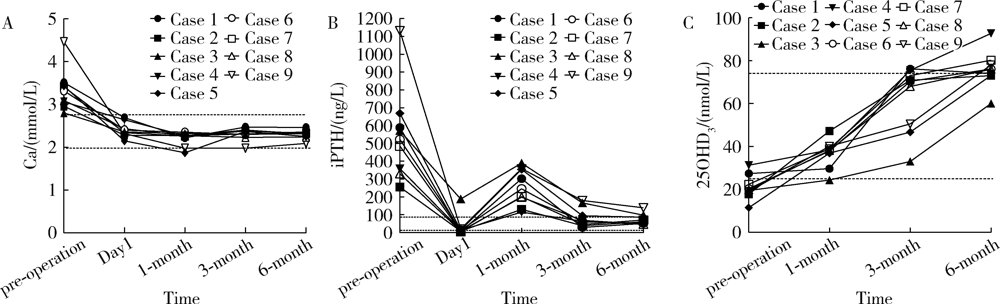
Normocalcemic with elevated post-operative parathormone in primary hyperpara-thyroidism: 9 case reports and literature review
XIE Ling-ding,WANG Na,ZHANG Jin-ping,WANG Xin,CHEN Xiao-ping,ZHANG Bo,BU ShiΔ( )
)
- Department of Endocrinology, China-Japanese Friendship Hospital, Beijing 100029, China
CLC Number:
- R582.1

| [1] |
Silverberg SJ, Clarke BL, Peacock M, et al. Current issues in the presentation of asymptomatic primary hyperparathyroidism: proceedings of the Fourth International Workshop[J]. J Clin Endocrinol Metab, 2014,99(10):3580-3594.
doi: 10.1210/jc.2014-1415 |
| [2] |
Sun B, Guo B, Wu B, et al. Characteristics, management, and outcome of primary hyperparathyroidism at a single clinical center from 2005 to 2016[J]. Osteoporos Int, 2018,29(3):635-642.
doi: 10.1007/s00198-017-4322-7 pmid: 29198075 |
| [3] |
Yao XA, Wei BJ, Jiang T, et al. The characteristics of clinical changes in primary hyperparathyroidism in Chinese patients[J]. J Bone Miner Metab, 2019,37(2):336-341.
doi: 10.1007/s00774-018-0922-3 |
| [4] | 中华医学会骨质疏松和骨矿盐疾病分会, 中华医学会内分泌分会代谢性骨病学组. 原发性甲状旁腺功能亢进症诊疗指南[J]. 中华骨质疏松和骨矿盐疾病杂志, 2014,7(3):187-198. |
| [5] |
Wei Y, Peng L, Li Y, et al. Clinical study on safety and efficacy of microwave ablation for primary hyperparathyroidism[J]. Korean J Radiol, 2020,21(5):572-581.
doi: 10.3348/kjr.2019.0593 |
| [6] |
Fan BQ, He XW, Chen HH, et al. US-guided microwave ablation for primary hyperparathyroidism: a safety and efficacy study[J]. Eur Radiol, 2019,29(10):5607-5616.
doi: 10.1007/s00330-019-06078-y |
| [7] |
Biskobing DM. Significance of elevated parathyroid hormone after parathyroidectomy[J]. Endocr Pract, 2010,16(1):112-117.
doi: 10.4158/EP09122.RA pmid: 19789155 |
| [8] |
Goldfarb M, Gondek S, Irvin GL, 3rd, et al. Normocalcemic parathormone elevation after successful parathyroidectomy: long-term analysis of parathormone variations over 10 years[J]. Surgery, 2011,150(6):1076-1084.
doi: 10.1016/j.surg.2011.09.017 pmid: 22136824 |
| [9] |
Carsello CB, Yen TW, Wang TS. Persistent elevation in serum parathyroid hormone levels in normocalcemic patients after parathyroidectomy: does it matter?[J]. Surgery, 2012,152(4):575-581.
doi: 10.1016/j.surg.2012.07.005 pmid: 23021134 |
| [10] |
Beyer TD, Solorzano CC, Prinz RA, et al. Oral vitamin D supplementation reduces the incidence of eucalcemic PTH elevation after surgery for primary hyperparathyroidism[J]. Surgery, 2007,141(6):777-783.
pmid: 17560254 |
| [11] |
Lang BH, Wong IY, Wong KP, et al. Eucalcemic parathyroid hormone elevation after parathyroidectomy for primary sporadic hyperparathyroidism: risk factors, trend, and outcome[J]. Ann Surg Oncol, 2012,19(2):584-590.
doi: 10.1245/s10434-011-1846-5 |
| [12] |
Duke WS, Kim AS, Waller JL, et al. Persistently elevated parathyroid hormone after successful parathyroid surgery[J]. Laryngoscope, 2017,127(7):1720-1723.
doi: 10.1002/lary.v127.7 |
| [13] |
Caldwell M, Laux J, Clark M, et al. Persistently elevated PTH after parathyroidectomy at one year: experience in a tertiary referral center[J]. J Clin Endocrinol Metab, 2019,104(10):4473-4480.
doi: 10.1210/jc.2019-00705 |
| [14] |
Westerdahl J, Valdemarsson S, Lindblom P, et al. Postoperative elevated serum levels of intact parathyroid hormone after surgery for parathyroid adenoma: sign of bone remineralization and decreased calcium absorption[J]. World J Surg, 2000,24(11):1323-1329.
pmid: 11038201 |
| [15] |
Cao S, Hu Y, Zhao Y, et al. A retrospective study of elevated post-operative parathormone in primary hyperparathyroid patients[J]. Oncotarget, 2017,8(60):101158-101164.
doi: 10.18632/oncotarget.v8i60 |
| [16] |
Nordenstrom E, Westerdahl J, Isaksson A, et al. Patients with elevated serum parathyroid hormone levels after parathyroidectomy: showing signs of decreased peripheral parathyroid hormone sensiti-vity[J]. World J Surg, 2003,27(2):212-215.
doi: 10.1007/s00268-002-6600-5 |
| [17] |
Mittendorf EA, McHenry CR. Persistent parathyroid hormone elevation following curative parathyroidectomy for primary hyperparathyroidism[J]. Arch Otolaryngol Head Neck Surg, 2002,128(3):275-279.
doi: 10.1001/archotol.128.3.275 |
| [18] |
Rianon N, Alex G, Callender G, et al. Preoperative serum osteocalcin may predict postoperative elevated parathyroid hormone in patients with primary hyperparathyroidism[J]. World J Surg, 2012,36(6):1320-1326.
doi: 10.1007/s00268-012-1432-4 pmid: 22278606 |
| [19] | Silverberg SJ, Gartenberg F, Jacobs TP, et al. Increased bone mineral density after parathyroidectomy in primary hyperparathyroidism[J]. J Clin Endocrinol Metab, 1995,80(3):729-734. |
| [20] |
Ning L, Sippel R, Schaefer S, et al. What is the clinical significance of an elevated parathyroid hormone level after curative surgery for primary hyperparathyroidism?[J]. Ann Surg, 2009,249(3):469-472.
doi: 10.1097/SLA.0b013e31819a6ded |
| [21] |
Wang TS, Ostrower ST, Heller KS. Persistently elevated parathyroid hormone levels after parathyroid surgery[J]. Surgery, 2005,138(6):1130-1135.
doi: 10.1016/j.surg.2005.08.026 |
| [22] |
Carty SE, Roberts MM, Virji MA, et al. Elevated serum parathormone level after “concise parathyroidectomy” for primary sporadic hyperparathyroidism[J]. Surgery, 2002,132(6):1086-1092.
doi: 10.1067/msy.2002.128479 |
| [23] |
Press D, Politz D, Lopez J, et al. The effect of vitamin D levels on postoperative calcium requirements, symptomatic hypocalcemia, and parathormone levels following parathyroidectomy for primary hyperparathyroidism[J]. Surgery, 2011,150(6):1061-1068.
doi: 10.1016/j.surg.2011.09.018 |
| [24] |
Aberg V, Norenstedt S, Zedenius J, et al. Health-related quality of life after successful surgery for primary hyperparathyroidism: no additive effect from vitamin D supplementation: results of a double-blind randomized study[J]. Eur J Endocrinol, 2015,172(2):181-187.
doi: 10.1530/EJE-14-0757 |
| [25] |
Norenstedt S, Pernow Y, Zedenius J, et al. Vitamin D supplementation after parathyroidectomy: effect on bone mineral density: a randomized double-blind study[J]. J Bone Miner Res, 2014,29(4):960-967.
doi: 10.1002/jbmr.v29.4 |
| [26] |
Rolighed L, Rejnmark L, Sikjaer T, et al. Vitamin D treatment in primary hyperparathyroidism: a randomized placebo controlled trial[J]. J Clin Endocrinol Metab, 2014,99(3):1072-1080.
doi: 10.1210/jc.2013-3978 |
| [27] |
Grubbs EG, Rafeeq S, Jimenez C, et al. Preoperative vitamin D replacement therapy in primary hyperparathyroidism: safe and beneficial?[J]. Surgery, 2008,144(6):852-858.
doi: 10.1016/j.surg.2008.06.032 |
| [28] |
de la Plaza Llamas R, Ramia Angel JM, Arteaga Peralta V, et al. Elevated parathyroid hormone levels after successful parathyroidectomy for primary hyperparathyroidism: a clinical review[J]. Eur Arch Otorhinolaryngol, 2018,275(3):659-669.
doi: 10.1007/s00405-017-4836-9 |
| [1] | Ting JING,Hua JIANG,Ting LI,Qianqian SHEN,Lan YE,Yindan ZENG,Wenxin LIANG,Gang FENG,Man-Yau Szeto Ignatius,Yumei ZHANG. Relationship between serum 25-hydroxyvitamin D and handgrip strength in middle-aged and elderly people in five cities of Western China [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 448-455. |
| [2] | Lei BAO,Xia-xia CAI,Ming-yuan ZHANG,Lei-lei REN. Effect of vitamin D3 on mild cognitive impairment in type 2 diabetic mice and its possible mechanism [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 587-592. |
| [3] | Xi-ya SUN,Yi-lu CHEN,Lin ZENG,Li-ying YAN,Jie QIAO,Rong LI,Xu ZHI. Correlation analysis of vitamin D level and anti-Müllerian hormone in infertile female and the role in predicting pregnancy outcome [J]. Journal of Peking University (Health Sciences), 2023, 55(1): 167-173. |
| [4] | HE Wei,YANG Si-wen,CHEN Juan,ZHU Xiao-jun,CHEN Zhi-zhong,MA Wen-jun. Effects of 275 nm and 310 nm ultraviolet irradiation on bone metabolism in ovariectomized osteoporotic rats [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 236-243. |
| [5] | Jian-mei ZOU,Li-jun WU,Cai-nan LUO,Ya-mei SHI,Xue WU. Relationship of serum 25- hydroxy vitamin D and systemic lupus erythematosus [J]. Journal of Peking University (Health Sciences), 2021, 53(5): 938-941. |
| [6] | LIU Kai-ning, MENG Huan-xin, HOU Jian-xia. Influence of vitamin D receptor FokⅠ polymorphism on expression of CYP24A1 in periodontal cells [J]. Journal of Peking University(Health Sciences), 2018, 50(1): 13-19. |
| [7] | CAO Xiao-Jing, HE Lu, MENG Huan-Xin, LI Peng, CHEN Zhi-Bin. Relationship between vitamin D receptor gene polymorphisms and chronic periodontitis [J]. Journal of Peking University(Health Sciences), 2015, 47(4): 697-702. |
|
||