Journal of Peking University (Health Sciences) ›› 2023, Vol. 55 ›› Issue (6): 1013-1021. doi: 10.19723/j.issn.1671-167X.2023.06.009
Previous Articles Next Articles
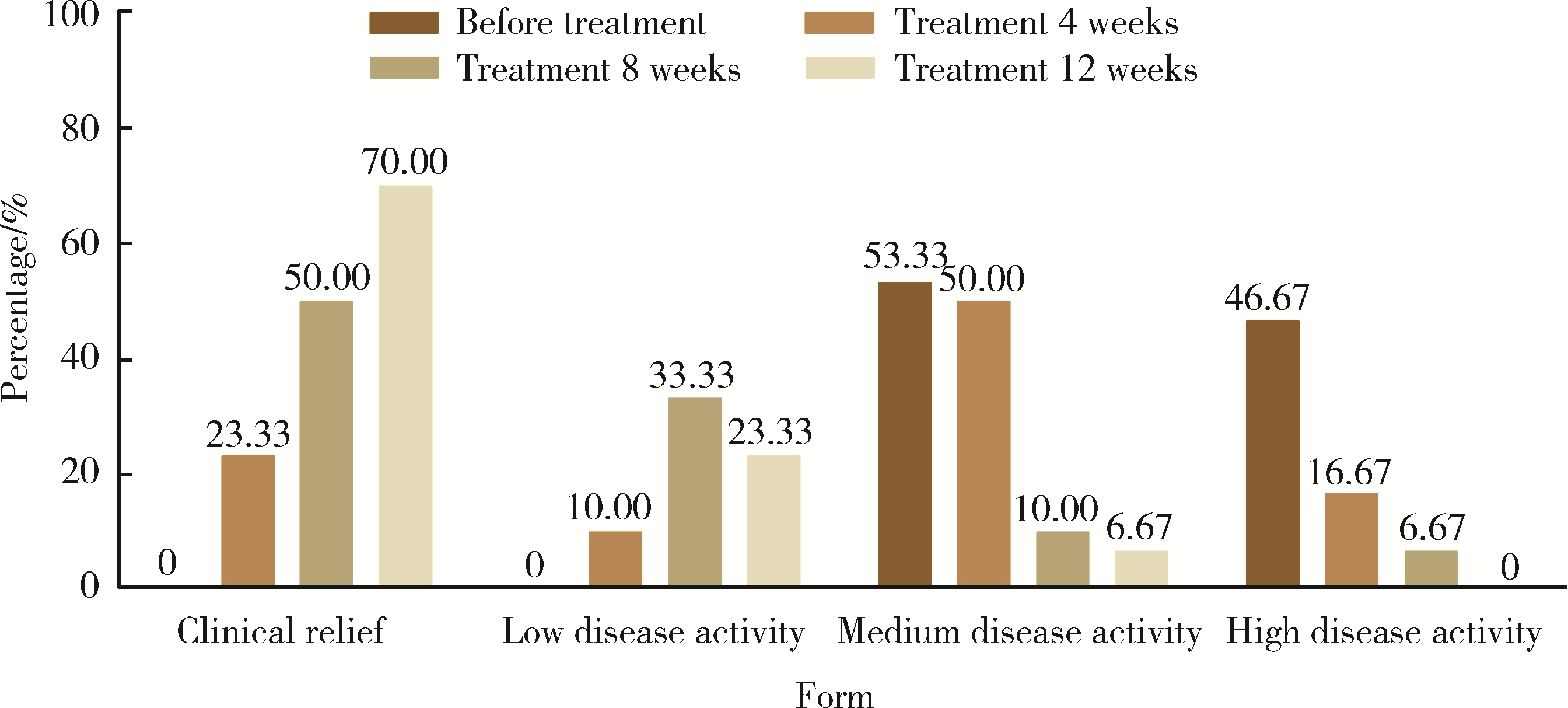
Effectiveness of tofacitinib combined with iguratimod in the treatment of difficult-to-treat moderate-to-severe rheumatoid arthritis
Xue ZOU1,2,Xiao-juan BAI1,Li-qing ZHANG1,*( )
)
- 1. Department of Rheumatology and Immunology, Fenyang Hospital Affiliated to Shanxi Medical University, Shanxi Province Fenyang Hospital, Fenyang 032200, Shanxi, China
2. Department of Gastroenterology, Suzhou Yongding Hospital, Suzhou 215100, Jiangsu, China
CLC Number:
- R593.22

| 1 |
Smolen JS , Landewé RBM , Bijlsma JWJ , et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying anti-rheumatic drugs: 2019 update[J]. Ann Rheum Dis, 2020, 79 (6): 685- 699.
doi: 10.1136/annrheumdis-2019-216655 |
| 2 | de Hair MJH , Jacobs JWG , Schoneveld JLM , et al. Difficult-to-treat rheumatoid arthritis: An area of unmet clinical need[J]. Rheumatology (Oxford), 2018, 57 (7): 1135- 1144. |
| 3 |
Buch MH . Defining refractory rheumatoid arthritis[J]. Ann Rheum Dis, 2018, 77 (7): 966- 969.
doi: 10.1136/annrheumdis-2017-212862 |
| 4 |
Smolen JS , Aletaha D , Mcinnes IB . Rheumatoid arthritis[J]. Lancet, 2016, 388 (10055): 2023- 2038.
doi: 10.1016/S0140-6736(16)30173-8 |
| 5 |
Aletaha D , Neogi T , Silman AJ , et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism Collaborative initiative[J]. Arthritis Rheum, 2010, 62 (9): 2569- 2581.
doi: 10.1002/art.27584 |
| 6 |
Wu D , Luo Y , Li T , et al. Systemic complications of rheumatoid arthritis: Focus on pathogenesis and treatment[J]. Front Immunol, 2022, 13, 1051082.
doi: 10.3389/fimmu.2022.1051082 |
| 7 |
Sun X , Li R , Cai Y , et al. Clinical remission of rheumatoid arthritis in a multi center real-world study in Asia-Pacific region[J]. Lancet Reg Health West Pac, 2021, 15, 100240.
doi: 10.1016/j.lanwpc.2021.100240 |
| 8 | 李宏超, 徐丽玲, 苏茵. 难治性类风湿关节炎诊治探讨[J]. 中华风湿病学杂志, 2019, 23 (10): 689- 693. |
| 9 |
Nagy G , Roodenrijs NMT , Welsing PM , et al. EULAR definition of difficult-to-treat rheumatoid arthritis[J]. Ann Rheum Dis, 2021, 80 (1): 31- 35.
doi: 10.1136/annrheumdis-2020-217344 |
| 10 |
Xie S , Li S , Tian J , et al. Iguratimod as a new drug for rheumatoid arthritis: Current landscape[J]. Front Pharmacol, 2020, 11, 73.
doi: 10.3389/fphar.2020.00073 |
| 11 | Xu Y , Zhu Q , Song J , et al. Regulatory effect of iguratimod on the balance of Th subsets and inhibition of inflammatory cytokines in patients with rheumatoid arthritis[J]. Mediators Inflamm, 2015, 2015, 356040. |
| 12 | Wen L , Jiang W , Zhou M , et al. Effect of combined application of iguratimod in the treatment of active rheumatoid arthritis on bone metabolism, Th17 cells and Treg cells[J]. Am J Transl Res, 2021, 13 (3): 1676- 1684. |
| 13 |
Liu S , Song LP , Li RB , et al. Iguratimod promotes transformation of mononuclear macrophages in elderly patients with rheumatoid arthritis by nuclear factor-κB pathway[J]. World J Clin Cases, 2021, 9 (10): 2181- 2191.
doi: 10.12998/wjcc.v9.i10.2181 |
| 14 |
Li CH , Ma ZZ , Jian LL , et al. Iguratimod inhibits osteoclastoge-nesis by modulating the RANKL and TNF-α signaling pathways[J]. Int Immunopharmacol, 2021, 90, 107219.
doi: 10.1016/j.intimp.2020.107219 |
| 15 |
Kondo N , Kuroda T , Kobayashi D . Cytokine networks in the pa-thogenesis of rheumatoid arthritis[J]. Int J Mol Sci, 2021, 22 (20): 10922.
doi: 10.3390/ijms222010922 |
| 16 | Malemud CJ . The role of the JAK/STAT signal pathway in rheumatoid arthritis[J]. Ther Adv Musculoskelet Dis, 2018, 10 (5/6): 117- 127. |
| 17 | 疏金玲, 张玲玲, 魏伟. 酪氨酸激酶抑制剂治疗类风湿关节炎研究进展[J]. 中国药理学与毒理学杂志, 2020, 34 (9): 713- 720. |
| 18 |
Puigdevall L , Michiels C , Stewardson C , et al. JAK/STAT: Why choose a classical or an alternative pathway when you can have both?[J]. J Cell Mol Med, 2022, 26 (7): 1865- 1875.
doi: 10.1111/jcmm.17168 |
| 19 | 戴冰冰, 刘佳丽, 李宁宁, 等. 托法替布治疗难治性中重度类风湿关节炎的疗效及安全性[J]. 实用临床医药杂志, 2022, 26 (11): 122- 126. |
| 20 |
Zheng N , Guo C , Wu R . Iguratimod is effective in refractory rheumatoid arthritis patients with inadequate response to metho-trexate-cyclosporin A-hydroxychloroquine-prednisone[J]. Scand J Rheumatol, 2018, 47 (5): 422- 424.
doi: 10.1080/03009742.2017.1376109 |
| 21 |
Mizutani S , Kodera H , Sato Y , et al. Clinical effectiveness of iguratimod based on real-world data of patients with rheumatoid arthritis[J]. Clin Rheumatol, 2021, 40 (1): 123- 132.
doi: 10.1007/s10067-020-05208-y |
| 22 | Inoue A , Nozaki Y , Hirooka Y , et al. The effectiveness and retention rate of iguratimod in Japanese rheumatoid arthritis patients with/without methotrexate in daily medical care[J]. Life (Basel), 2020, 10 (11): 261. |
| 23 | Ouyang D , Ma YZ , Zou J , et al. Effectiveness and safety of iguratimod monotherapy or combined with methotrexate in treating rheumatoid arthritis: A aystematic review and meta-analysis[J]. Front Pharmacol, 2022, 13, 911810. |
| 24 | Smolen JS , Landewe R , Breedveld FC , et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update[J]. Ann Rheum Dis, 2014, 73 (3): 492- 509. |
| 25 | Angelini J , Talotta R , Roncato R , et al. JAK-inhibitors for the treatment of rheumatoid arthritis: A focus on the present and an outlook on the future[J]. Biomolecules, 2020, 10 (7): 1002. |
| 26 | 张春燕, 范小冬, 秦元, 等. JAK抑制剂托法替布治疗类风湿性关节炎效果的Meta分析[J]. 第三军医大学学报, 2018, 40 (6): 543- 550. |
| 27 | Sands BE , Taub PR , Armuzzi A , et al. Tofacitinib treatment is associated with modest and reversible increases in serum lipids in patients with ulcerative colitis[J]. Clin Gastroenterol Hepatol, 2020, 18 (1): 123- 132.e3. |
| 28 | Taylor PC , Kremer JM , Emery P , et al. Lipid profile and effect of statin treatment in pooled phase Ⅱ and phase Ⅲ baricitinib studies[J]. Ann Rheum Dis, 2018, 77 (7): 988- 995. |
| [1] | Zhaode BU, Mengyu FENG, Ke JI. Practice and reflection on sentinel lymph node navigation surgery for early gastric cancer [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 239-243. |
| [2] | Youdong LIU, Yajun LYU, Jie CHEN, Mingde ZANG, Hongda PAN, Xiaowen LIU, Jun LU, Fenglin LIU. Clinical efficacy and safety of totally laparoscopic subtotal gastrectomy with cardia-gastric fundus preservation in middle-upper gastric cancer [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 301-306. |
| [3] | Hui WEI, Jingfeng ZHANG, Zhongqiang YAO, Jinxia ZHAO. Clinical characteristics and relevant factors of rheumatoid arthritis patients with anemia of chronic disease [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 307-312. |
| [4] | Weihao LI, Xuemin ZHANG, Wei LI, Tao ZHANG, Xiaoming ZHANG. Outcomes of suture-mediated vascular closure device in the closure of left brachial artery access site after thoracic endovascular aortic repair [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 388-392. |
| [5] | Ebrahimi Farin, Zhiqiang FENG, Ebrahimi Faraz, Weihua HAN, Ziyang YU, Kuankuan JIA, Jingang AN. Surgical treatment outcomes of different stages of maxillary medication-related osteonecrosis of the jaw [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 107-114. |
| [6] | Lianfei PAN, Wenjing LI, Ruiyang WANG, Jian JIAO, Zhanqiang CAO, Li GAO, Dong SHI. Short-term efficacy and influencing factors of systemic antibiotics as an adjunct to mechanical periodontal therapy for stages Ⅲ/Ⅳ periodontitis [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 30-36. |
| [7] | Tao WU, Jianzi LIN, Yafeng ZHU, Jianda MA, Peiwen JIA, Lijuan YANG, jie PAN, Yaowei ZOU, Ying YANG, Ye LU, Lie DAI. Serum inter-alpha-trypsin inhibitor heavy chain H3 is identified as a potential biomarker for myopenia in patients with rheumatoid arthritis using proteomic profiling [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1024-1031. |
| [8] | Yan DING, Lifang WANG, Chaoran LI, Zhemin LU, Lianjie SHI. Rheumatoid arthritis combined with IgG4-related disease successfully treated with rituximab: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1203-1207. |
| [9] | Ju YANG, Jing XU, Juhua DAI, Lianjie SHI. Expression of lumican protein in serum of patients with rheumatoid arthritis and its correlation with disease and immune activities [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 911-918. |
| [10] | Lianghua FENG, Lirong HONG, Yujia CHEN, Xueming CAI. Role and mechanism of ubiquitin-specific protease 35 in ferroptosis of rheumatoid arthritis-fibroblast like synoviocytes [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 919-925. |
| [11] | Yuanyuan YANG, Shanshan ZHANG, Guangyan YU, Huijun YANG, Hongyu YANG. Clinical outcomes of partial sialoadenectomy for the treatment of benign tumors in the submandibular gland [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 334-339. |
| [12] | Yifan KANG, Yanjun GE, Xiaoming LV, Shang XIE, Xiaofeng SHAN, Zhigang CAI. One-stage mandibular reconstruction combining iliac flap with immediate implant-based denture [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 78-84. |
| [13] | Peiwen JIA, Ying YANG, Yaowei ZOU, Zhiming OUYANG, Jianzi LIN, Jianda MA, Kuimin YANG, Lie DAI. Clinical characteristics of overlapping syndromes of low muscle mass in patients with rheumatoid arthritis and their impact on physical function [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1009-1016. |
| [14] | Doudou MA, Zhemin LU, Qian GUO, Sha ZHU, Jin GU, Yan DING, Lianjie SHI. Successful treatment of rheumatoid arthritis complicated with myasthenia gravis with low-dose rituximab: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1110-1114. |
| [15] | Rui YAN, Dan KE, Yan ZHANG, Li LI, Huanran SU, Wei CHEN, Mingxia SUN, Xiaomin LIU, Liang LUO. Diagnostic significance of serum chemokine CXCL-10 and Krebs von den lungen-6 level in patients with rheumatoid arthritis associated interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 956-962. |
|
||