Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (1): 204-209. doi: 10.19723/j.issn.1671-167X.2021.01.031
Previous Articles Next Articles
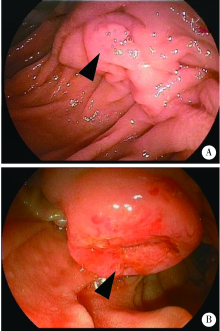
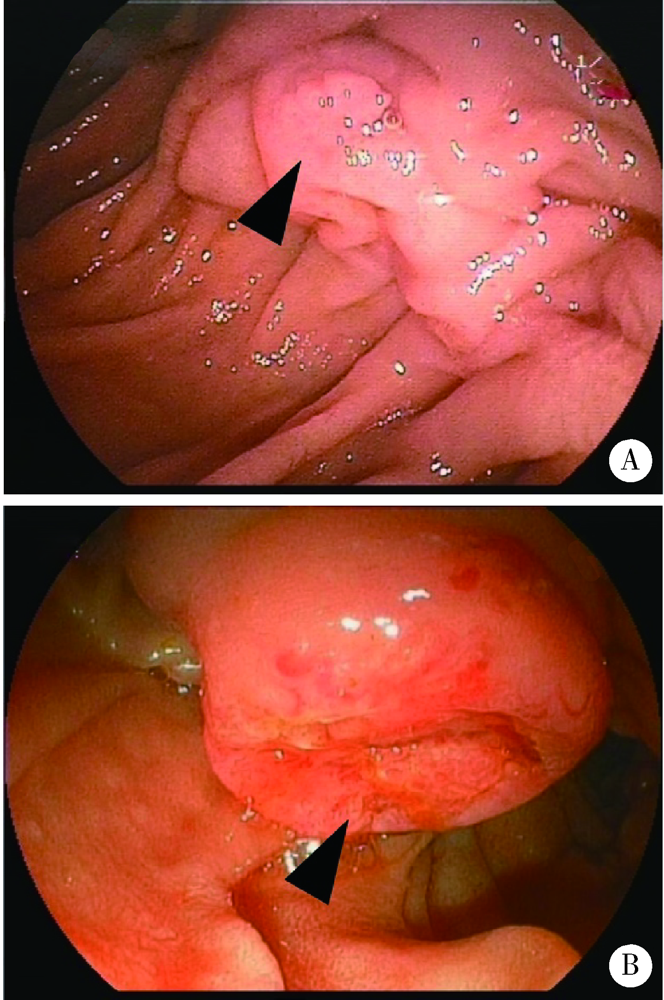
Characteristics of benign and malignant lesions of ampullary polyps and the accuracy of forceps biopsy
WANG Ying-chun,HUANG Yong-hui( ),CHANG Hong,YAO Wei,YAN Xiu-e,LI Ke,ZHANG Yao-peng,ZHENG Wei
),CHANG Hong,YAO Wei,YAN Xiu-e,LI Ke,ZHANG Yao-peng,ZHENG Wei
- Department of Gastroenterology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R574.51


| [1] |
Ridtitid W, Tan D, Schmidt SE, et al. Endoscopic papillectomy: risk factors for incomplete resection and recurrence during long-term follow-up[J]. Gastrointest Endosc, 2014,79(2):289-296.
pmid: 24094466 |
| [2] |
Ridtitid W, Schmidt SE, Al-Haddad MA, et al. Performance characteristics of EUS for locoregional evaluation of ampullary lesions[J]. Gastrointest Endosc, 2015,81(2):380-388.
doi: 10.1016/j.gie.2014.08.005 pmid: 25293823 |
| [3] |
Kang SH, Kim KH, Kim TN, et al. Therapeutic outcomes of endoscopic papillectomy for ampullary neoplasms: retrospective analysis of a multicenter study[J]. BMC Gastroenterol, 2017,17(1):69.
doi: 10.1186/s12876-017-0626-5 pmid: 28558658 |
| [4] |
El H, Coté GA. Endoscopic diagnosis and management of ampullary lesions[J]. Gastrointest Endosc Clin N Am, 2013,23(1):95-109.
doi: 10.1016/j.giec.2012.10.004 pmid: 23168121 |
| [5] | 顾宗廷, 张永杰. 十二指肠乳头肿瘤的诊断与外科治疗[J]. 国际消化病杂志, 2015,35(6):428-435. |
| [6] |
Chathadi KV, Khashab MA, Acosta RD, et al. The role of endoscopy in ampullary and duodenal adenomas[J]. Gastrointest Endosc, 2015,82(5):773-781.
doi: 10.1016/j.gie.2015.06.027 pmid: 26260385 |
| [7] | 陆鉴, 陆文洁, 吴育连. 十二指肠乳头肿瘤的临床特点及诊治分析[J]. 中华外科杂志, 2016,54(3):187-190. |
| [8] |
Attila T, Parlak E, Alper E, et al. Endoscopic papillectomy of benign ampullary lesions: Outcomes from a multicenter study[J]. Turk J Gastroenterol, 2018,29(3):325-334.
doi: 10.5152/tjg.2018.17378 pmid: 29755017 |
| [9] |
Wanders LK, East JE, Uitentuis SE, et al. Diagnostic performance of narrowed spectrum endoscopy, autofluorescence imaging, and confocal laser endomicroscopy for optical diagnosis of colonic polyps: a meta-analysis[J]. Lancet Oncol, 2013,14(13):1337-1347.
doi: 10.1016/S1470-2045(13)70509-6 pmid: 24239209 |
| [10] |
Kim HN, Kim KM, Shin JU, et al. Prediction of carcinoma after resection in subjects with ampullary adenomas on endoscopic biopsy[J]. J Clin Gastroenterol, 2013,47(4):346-351.
doi: 10.1097/MCG.0b013e318272f2ef pmid: 23442830 |
| [11] | 郝璐, 王伟, 施新岗, 等. 十二指肠乳头肿瘤内镜切除术的临床应用进展[J]. 中华消化内镜杂志, 2017,34(6):451-454. |
| [12] |
Wee E, Lakhtakia S, Gupta R, et al. The diagnostic accuracy and strength of agreement between endoscopic ultrasound and histopathology in the staging of ampullary tumors[J]. Indian J Gastroenterol, 2012,31(6):324-332.
doi: 10.1007/s12664-012-0248-3 pmid: 22996048 |
| [13] | 张荣春, 陈杰, 于卫华, 等. 十二指肠乳头肿瘤内镜切除术[J]. 中华消化内镜杂志, 2014,31(4):231-235. |
| [14] |
Bourgeois N, Dunham F, Verhest A, et al. Endoscopic biopsies of the papilla of Vater at the time of endoscopic sphincterotomy: difficulties in interpretation[J]. Gastrointest Endosc, 1984,30(3):163-166.
doi: 10.1016/s0016-5107(84)72357-1 pmid: 6735092 |
| [1] | Hui WEI, Jingfeng ZHANG, Zhongqiang YAO, Jinxia ZHAO. Clinical characteristics and relevant factors of rheumatoid arthritis patients with anemia of chronic disease [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 307-312. |
| [2] | Jie ZHAO, Chun FU, Xiujuan ZHAO, Haiyan XUE, Shu LI, Zhenzhou WANG, Fengxue ZHU. Risk factors for ventilator-associated pneumonia in patients with chest trauma in intensive care unit [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 351-358. |
| [3] | Jialin LI, Liqiao CHEN, Jiatian TANG, Yan WU, Anqiang WANG. Conversion therapy for hepatoid adenocarcinoma of the stomach: A case report [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 399-404. |
| [4] | Xiaolin WANG, Luyao LI, Wen ZHANG, Hongyan WANG. Clinicopathological analysis of mesonephric-like adenocarcinoma in the corpusuteri: A report of 3 cases [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1208-1212. |
| [5] | Weihua HOU, Shujie SONG, Zhongyue SHI, Lu LIU, Mulan JIN. Neuroendocrine carcinoma with significantly vacuolar nucleus at the esophagogastric junction: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 1005-1009. |
| [6] | Bowen LI, Qiang ZHANG, Yixin SUN. Establishment and validation of a risk prediction model for scoliosis after Nuss procedure in children and young adults with pectus excavatum [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 941-946. |
| [7] | Xiaoyong YANG, Fan ZHANG, Lulin MA, Cheng LIU. Clinical characteristics and influencing factors of extraglandular invasion of prostatic ductal adenocarcinoma [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 956-960. |
| [8] | Wei LIU, Wen GUO, Zhe GUO, Chunyan LI, Yunlong LI, Siqi LIU, Liang ZHANG, Hui SONG. Risk factors associated with non-radiographic bone erosion in patients with gout [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 735-739. |
| [9] | Mengxi LU, Qiuping LIU, Tianjing ZHOU, Xiaofei LIU, Yexiang SUN, Peng SHEN, Hongbo LIN, Xun TANG, Pei GAO. Association of triglyceride-glucose index and cardiovascular disease in a community-based Chinese cohort [J]. Journal of Peking University (Health Sciences), 2025, 57(3): 430-435. |
| [10] | Dan HAN, Yangjin CIREN, Qiuhong LI, Jun LI. Changes of intestinal microflora in patients with colorectal benign and malignant tumors in high altitude area and comparison with the normal population in low altitude area [J]. Journal of Peking University (Health Sciences), 2025, 57(3): 578-583. |
| [11] | Huaqiu GUO, Zhe WANG, Xue YANG, Jie BAI. Clinical features and risk factors of patients with oral bleeding in dental emergency [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 142-147. |
| [12] | Minting DENG, Nan WANG, Bin XIA, Yuming ZHAO, Junxia ZHU. Factors associated with spontaneous re-eruption of traumatically intruded permanent anterior teeth in children and adolescents [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 148-153. |
| [13] | Yukai LI, Hongyan WANG, Liang LUO, Yun LI, Chun LI. Clinical significance of antiphospholipid antibodies in Behcet disease with thrombosis [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1036-1040. |
| [14] | Yang TIAN, Yongzheng HAN, Jiao LI, Mingya WANG, Yinyin QU, Jingchao FANG, Hui JIN, Min LI, Jun WANG, Mao XU, Shenglin WANG, Xiangyang GUO. Incidence and risk factors of postoperative epidural hematoma following anterior cervical spine surgery [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1058-1064. |
| [15] | Mingrui WANG, Jinhui LAI, Jiaxiang JI, Xinwei TANG, Haopu HU, Qi WANG, Kexin XU, Tao XU, Hao HU. Risk factors for decreased quality of life in patients with kidney stones predicted by the Chinese version of Wisconsin stone quality of life questionnaire [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1069-1074. |
|
||