Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (6): 1133-1138. doi: 10.19723/j.issn.1671-167X.2021.06.021
Previous Articles Next Articles
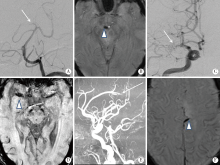
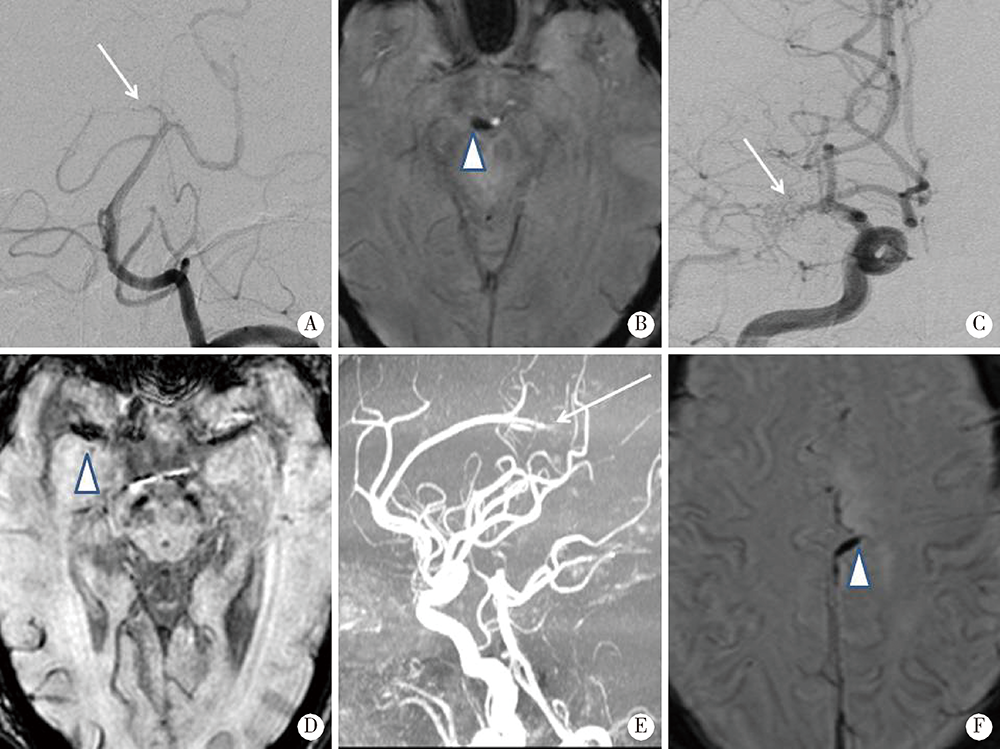
Susceptibility vessel sign in subacute stroke patients with large vessel occlusion
REN Guo-yong1,2,WU Xue-mei2, 1,LI Jie-yu1,SUN Wei-ping1,△( ),HUANG Yi-ning1
),HUANG Yi-ning1
- 1. Department of Neurology, Peking University First Hospital, Beijing 100034, China
2. Department of Neurology, General Hospital of Taiyuan Iron & Steel CO., LTD.(TISCO), Taiyuan 030003, China]
CLC Number:
- R741
| [1] |
Gorelick PB, Wong KS, Bae HJ, et al. Large artery intracranial occlusive disease: A large worldwide burden but a relatively neglected frontier[J]. Stroke, 2008, 39(8):2396-2399.
doi: 10.1161/STROKEAHA.107.505776 pmid: 18535283 |
| [2] |
Ornello R, Degan D, Tiseo C, et al. Distribution and temporal trends from 1993 to 2015 of ischemic stroke subtypes: A systematic review and meta-analysis[J]. Stroke, 2018, 49(4):814-819.
doi: 10.1161/STROKEAHA.117.020031 |
| [3] |
Tian C, Cao X, Wang J. Recanalisation therapy in patients with acute ischaemic stroke caused by large artery occlusion: Choice of therapeutic strategy according to underlying aetiological mechanism[J]. Stroke Vasc Neurol, 2017, 2(4):244-250.
doi: 10.1136/svn-2017-000090 |
| [4] |
Allibert R, Billon GC, Vuillier F, et al. Advantages of susceptibility-weighted magnetic resonance sequences in the visualization of intravascular thrombi in acute ischemic stroke[J]. Int J Stroke, 2014, 9(8):980-984.
doi: 10.1111/ijs.12373 pmid: 25319168 |
| [5] |
Cho KH, Kim JS, Kwon SU, et al. Significance of susceptibility vessel sign on T2*-weighted gradient echo imaging for identification of stroke subtypes[J]. Stroke, 2005, 36(11):2379-2383.
doi: 10.1161/01.STR.0000185932.73486.7a |
| [6] |
Horie N, Tateishi Y, Morikawa M, et al. Acute stroke with major intracranial vessel occlusion: Characteristics of cardioembolism and atherosclerosis-related in situ stenosis/occlusion[J]. J Clin Neurosci, 2016, 32(8):24-29.
doi: 10.1016/j.jocn.2015.12.043 |
| [7] |
Kang DW, Jeong HG, Kim DY, et al. Prediction of stroke subtype and recanalization using susceptibility vessel sign on susceptibility-weighted magnetic resonance imaging[J]. Stroke, 2017, 48(6):1554-1559.
doi: 10.1161/STROKEAHA.116.016217 |
| [8] |
Bourcier R, Derraz I, Delasalle B, et al. Susceptibility vessel sign and cardioembolic etiology in the THRACE trial[J]. Clin Neuroradiol, 2019, 29(4):685-692.
doi: 10.1007/s00062-018-0699-8 pmid: 29947813 |
| [9] |
Adams HP, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of org 10172 in acute stroke treatment[J]. Stroke, 1993, 24(1):35-41.
pmid: 7678184 |
| [10] |
Mori E, Yoneda Y, Tabuchi M, et al. Intravenous recombinant tissue plasminogen activator in acute carotid artery territory stroke[J]. Neurology, 1992, 42(5):976-982.
pmid: 1579252 |
| [11] |
Molina CA, Montaner J, Abilleira S, et al. Timing of spontaneous recanalization and risk of hemorrhagic transformation in acute cardioembolic stroke[J]. Stroke, 2001, 32(5):1079-1084.
pmid: 11340213 |
| [12] |
Fitzgerald S, Dai D, Wang S, et al. Platelet-rich emboli in cerebral large vessel occlusion are associated with a large artery atherosclerosis source[J]. Stroke, 2019, 50(7):1907-1910.
doi: 10.1161/STROKEAHA.118.024543 pmid: 31138084 |
| [13] |
Sato Y, Ishibashi-Ueda H, Iwakiri T, et al. Thrombus components in cardioembolic and atherothrombotic strokes[J]. Thromb Res, 2012, 130(2):278-280.
doi: 10.1016/j.thromres.2012.04.008 |
| [14] | 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国缺血性脑卒中和短暂性脑缺血发作二级预防指南2014[J]. 中华神经科杂志, 2015, 48(4):258-273. |
| [15] | Patel AR, Patel AR, Desai S. The underlying stroke etiology: A comparison of two classifications in a rural setup[J]. Cureus, 2019, 11(7):51-57. |
| [16] | Radbruch A, Mucke J, Schweser F, et al. Comparison of susceptibility weighted imaging and TOF-angiography for the detection of thrombi in acute stroke[J]. PLoS One, 2013, 8(5):634-639. |
| [1] | Jingxian WU, Liuyan ZHENG, Huan YU, Huairong WANG, Shuting XIE, Yalin CHEN, Teng LI, Mengying WANG, Xueying QIN, Tao WU, Dafang CHEN, Yiqun WU, Yonghua HU. Association analysis between genetic nurturing effects of CTNNA gene family and ischemic stroke [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 528-535. |
| [2] | Qingwei MENG, Meng FAN, Huangda GUO, Hanyu ZHANG, Mengying WANG, Siyue WANG, Hexiang PENG, Xueheng WANG, Tianjiao HOU, Xueying QIN, Dafang CHEN, Jing LI, Yiqun WU, Tao WU, Hongbo CHEN, Yonghua HU. Prognostic analysis of anticoagulation therapy in elderly patients with cardioembolic stroke [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 536-542. |
| [3] | Kun WANG, Huairong WANG, Huan YU, Ruotong YANG, Liuyan ZHENG, Jingxian WU, Xueying QIN, Tao WU, Dafang CHEN, Yiqun WU, Yonghua HU. Identifying genetic etiology of ischemic stroke based on pleiotropy of obesity related genes: A sibling study [J]. Journal of Peking University (Health Sciences), 2025, 57(3): 448-455. |
| [4] | Huan YU,Ruo-tong YANG,Si-yue WANG,Jun-hui WU,Meng-ying WANG,Xue-ying QIN,Tao WU,Da-fang CHEN,Yi-qun WU,Yong-hua HU. Metformin use and risk of ischemic stroke in patients with type 2 diabetes: A cohort study [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 456-464. |
| [5] | Yu-han DENG,Yong JIANG,Zi-yao WANG,Shuang LIU,Yu-xin WANG,Bao-hua LIU. Long short-term memory and Logistic regression for mortality risk prediction of intensive care unit patients with stroke [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 458-467. |
| [6] | Ruo-tong YANG,Meng-ying WANG,Chun-nan LI,Huan YU,Xiao-wen WANG,Jun-hui WU,Si-yue WANG,Jia-ting WANG,Da-fang CHEN,Tao WU,Yong-hua HU. Interaction between ischemic stroke risk loci identified by genome-wide association studies and sleep habits [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 412-420. |
| [7] | WU Jun-hui,WU Yi-qun,WU Yao,WANG Zi-jing,WU Tao,QIN Xue-ying,WANG Meng-ying,WANG Xiao-wen,WANG Jia-ting,HU Yong-hua. Incidence and risk factors of ischemic stroke in patients with type 2 diabetes among urban workers in Beijing, China [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 249-254. |
| [8] | Ya-fei LIU,Lin-lin SONG,Mao-wei XING,Li-xin CAI,Dong-xin WANG. Comparison of pulse pressure variation, stroke volume variation, and plethysmographic variability index in pediatric patients undergoing craniotomy [J]. Journal of Peking University (Health Sciences), 2021, 53(5): 946-951. |
| [9] | Yue HOU,Xu-tong ZHAO,Zhi-ying XIE,Yun YUAN,Zhao-xia WANG. Mitochondrial encephalopathy, lactic acidosis and stroke-like episodes / myoclonus epilepsy with ragged-red fibers /Leigh overlap syndrome caused by mitochondrial DNA 8344A>G mutation [J]. Journal of Peking University (Health Sciences), 2020, 52(5): 851-855. |
| [10] | Xun TANG,Du-dan ZHANG,Xiao-fei LIU,Qiu-ping LIU,Yang CAO,Na LI,Shao-ping HUANG,Hui-dong DOU,Pei GAO,Yong-hua HU. Application of the China-PAR stroke risk equations in a rural northern Chinese population [J]. Journal of Peking University (Health Sciences), 2020, 52(3): 444-450. |
| [11] | Zi-chang JIA,Huan-ju BIAN,Xuan LI,Jing-yuan LUAN,Chang-ming WANG,Qi-jia LIU,Jin-tao HAN. Application of Neuroform EZ stent in the treatment of severe intracranial arterial stenosis with complex symptomatic [J]. Journal of Peking University(Health Sciences), 2019, 51(5): 835-839. |
| [12] | Zi-chang JIA,Xuan LI,Xiao-gang LI,Xiang-zhu ZENG,Jing-yuan LUAN,Chang-ming WANG,Jin-tao HAN. Mechanical thrombectomy treatment in patients with acute ischemic stroke: a single center study [J]. Journal of Peking University(Health Sciences), 2019, 51(2): 256-259. |
| [13] | SUN Zhuo-nan, MENG Xiu-li, WANG Jun, GUO Xiang-yang, HAN Jin-tao, QI Qiang. Perioperative stroke effectively treated by an acute stroke team including anesthesia department: a case report [J]. Journal of Peking University(Health Sciences), 2017, 49(6): 1090-1094. |
| [14] | XIAO Tian-yi, LIU Yan, LI Ji-lai, WANG Rui-tong, DU Ji-chen. Diagnostic value of carotid atherosclerosis score for ischemic stroke [J]. Journal of Peking University(Health Sciences), 2016, 48(6): 1000-1005. |
| [15] | YU Can-qing, CHEN Yi-ping, LV Jun, GUO Yu, Paul SHERLIKER, BIAN Zheng, ZHOU Hui-yan, TAN Yun-long, CHEN Jun-shi, CHEN Zheng-ming, LI Li-ming1. Major depressive disorder in relation with coronary heart disease and stroke in Chinese adults aged 30-79 years [J]. Journal of Peking University(Health Sciences), 2016, 48(3): 465-471. |
|
||