Journal of Peking University (Health Sciences) ›› 2023, Vol. 55 ›› Issue (5): 818-824. doi: 10.19723/j.issn.1671-167X.2023.05.007
Previous Articles Next Articles
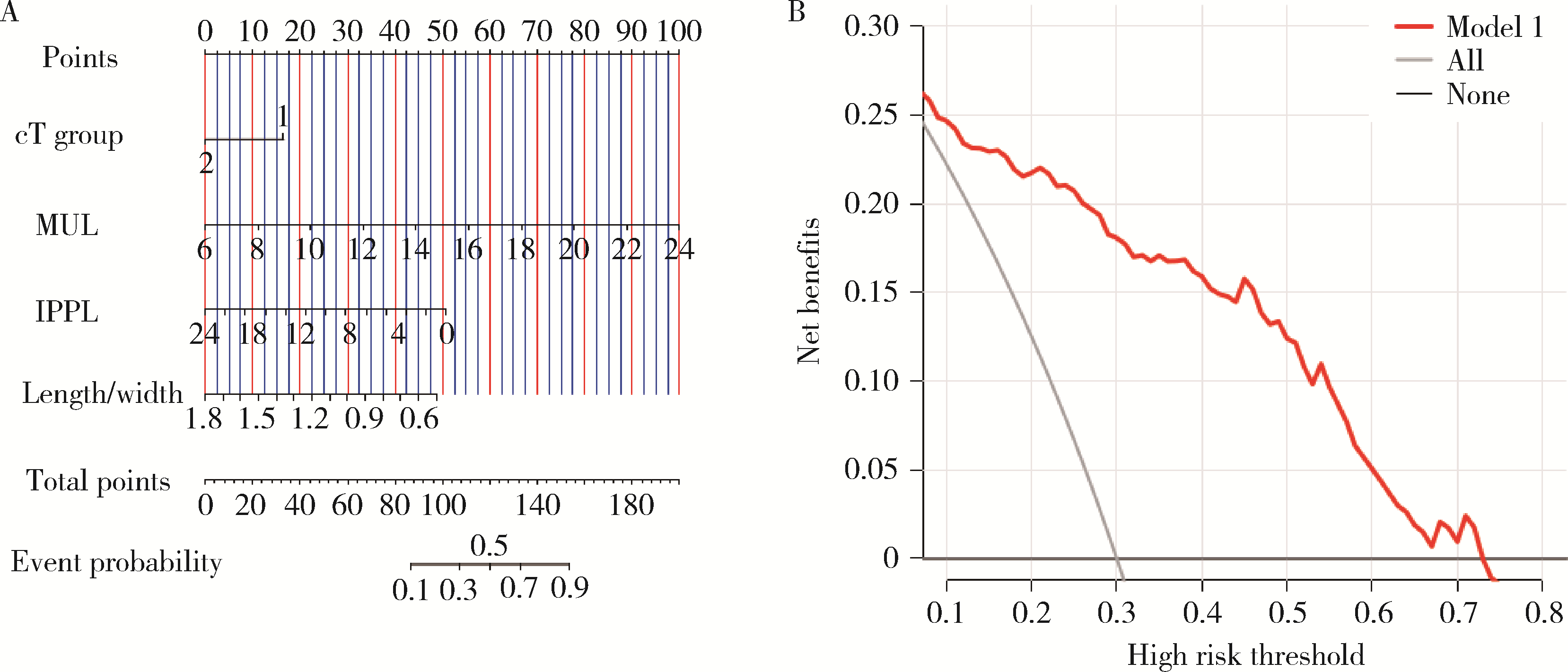
Predictive model of early urinary continence recovery based on prostate gland MRI parameters after laparoscopic radical prostatectomy
Hai MAO1,2,Fan ZHANG1,Zhan-yi ZHANG1,Ye YAN1,Yi-chang HAO1,Yi HUANG1,*( ),Lu-lin MA1,Hong-ling CHU3,*(),Shu-dong ZHANG1
),Lu-lin MA1,Hong-ling CHU3,*(),Shu-dong ZHANG1
- 1. Department of Urology, Peking University Third Hospital, Beijing 100191, China
2. Department of Urology, Traditional Chinese Medicine Hospital of Fengjie, Fengjie 404600, Chongqing, China
3. Research Center of Clinical Epidemiology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R737.25

| 1 |
Mottet N , van den Bergh RCN , Briers E , et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 update. Part 1: Screening, diagnosis, and local treatment with curative intent[J]. Eur Urol, 2021, 79 (2): 243- 262.
doi: 10.1016/j.eururo.2020.09.042 |
| 2 |
Ficarra V , Novara G , Rosen RC , et al. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy[J]. Eur Urol, 2012, 62 (3): 405- 417.
doi: 10.1016/j.eururo.2012.05.045 |
| 3 |
Adam M , Tennstedt P , Lanwehr D , et al. Functional outcomes and quality of life after radical prostatectomy only versus a combination of prostatectomy with radiation and hormonal therapy[J]. Eur Urol, 2017, 71 (3): 330- 336.
doi: 10.1016/j.eururo.2016.11.015 |
| 4 |
Heesakkers J , Farag F , Bauer RM , et al. Pathophysiology and contributing factors in postprostatectomy incontinence: A review[J]. Eur Urol, 2017, 71 (6): 936- 944.
doi: 10.1016/j.eururo.2016.09.031 |
| 5 |
Lamberg H , Shankar PR , Singh K , et al. Preoperative prostate MRI predictors of urinary continence following radical prostatectomy[J]. Radiology, 2022, 303 (1): 99- 109.
doi: 10.1148/radiol.210500 |
| 6 |
van Dijk-de Haan MC , Boellaard TN , Tissier R , et al. Value of different magnetic resonance imaging-based measurements of anatomical structures on preoperative prostate imaging in predicting urinary continence after radical prostatectomy in men with prostate cancer: A systematic review and meta-analysis[J]. Eur Urol Focus, 2022, 8 (5): 1211- 1225.
doi: 10.1016/j.euf.2022.01.015 |
| 7 |
Mungovan SF , Sandhu JS , Akin O , et al. Preoperative membranous urethral length measurement and continence recovery following radical prostatectomy: A systematic review and meta-analysis[J]. Eur Urol, 2017, 71 (3): 368- 378.
doi: 10.1016/j.eururo.2016.06.023 |
| 8 |
Manfredi M , Checcucci E , Fiori C , et al. Total anatomical reconstruction during robot-assisted radical prostatectomy: Focus on urinary continence recovery and related complications after 1 000 procedures[J]. BJU Int, 2019, 124 (3): 477- 486.
doi: 10.1111/bju.14716 |
| 9 |
Matsushita K , Kent MT , Vickers AJ , et al. Preoperative predictive model of recovery of urinary continence after radical prostatectomy[J]. BJU Int, 2015, 116 (4): 577- 583.
doi: 10.1111/bju.13087 |
| 10 |
Tutolo M , Bruyneel L , van der Aa F , et al. A novel tool to predict functional outcomes after robot-assisted radical prostatectomy and the value of additional surgery for incontinence[J]. BJU Int, 2021, 127 (5): 575- 584.
doi: 10.1111/bju.15242 |
| 11 |
Lee SE , Byun SS , Lee HJ , et al. Impact of variations in prostatic apex shape on early recovery of urinary continence after radical retropubic prostatectomy[J]. Urology, 2006, 68 (1): 137- 141.
doi: 10.1016/j.urology.2006.01.021 |
| 12 |
Walz J , Epstein JI , Ganzer R , et al. A critical analysis of the current knowledge of surgical anatomy of the prostate related to optimisation of cancer control and preservation of continence and erection in candidates for radical prostatectomy: An update[J]. Eur Urol, 2016, 70 (2): 301- 311.
doi: 10.1016/j.eururo.2016.01.026 |
| 13 | Zhang F , Chu H , Hao Y , et al. Preoperative predictive model of early urinary continence recovery after laparoscopic radical prostatectomy[J]. World J Urol, 2023, 41 (1): 59- 65. |
| 14 |
Kadono Y , Nohara T , Kawaguchi S , et al. Investigating the me-chanism underlying urinary continence recovery after radical prostatectomy: Effectiveness of a longer urethral stump to prevent urinary incontinence[J]. BJU Int, 2018, 122 (3): 456- 462.
doi: 10.1111/bju.14181 |
| 15 |
Nunez Bragayrac LA , Hussein AA , Attwood K , et al. Feasibility and continence outcomes of extended prostatic urethral preservation during robot-assisted radical prostatectomy[J]. Prostate Cancer Prostatic Dis, 2020, 23 (2): 286- 294.
doi: 10.1038/s41391-019-0173-y |
| 16 |
Huang AC , Kowalczyk KJ , Hevelone ND , et al. The impact of prostate size, median lobe, and prior benign prostatic hyperplasia intervention on robot-assisted laparoscopic prostatectomy: Technique and outcomes[J]. Eur Urol, 2011, 59 (4): 595- 603.
doi: 10.1016/j.eururo.2011.01.033 |
| 17 |
Jo JK , Hong SK , Byun SS , et al. Urinary Continence after robot-assisted laparoscopic radical prostatectomy: The impact of intrave-sical prostatic protrusion[J]. Yonsei Med J, 2016, 57 (5): 1145- 1151.
doi: 10.3349/ymj.2016.57.5.1145 |
| 18 |
Hoeh B , Wenzel M , Müller M , et al. Urethral sphincter length but not prostatic apex shape in preoperative MRI is associated with mid-term continence rates after radical prostatectomy[J]. Diagnostics (Basel), 2022, 12 (3): 701.
doi: 10.3390/diagnostics12030701 |
| [1] | Nannan WANG, Dajin YUAN, Yubing ZHU, Lei DING. Development and validation of a multicenter nomogram predicting the risk of liver metastasis after curative resection of colorectal cancer [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 290-300. |
| [2] | Zhemin LI, Jiafu JI, Guoxin LI, Ziyu LI, Zhaode BU, Xiangyu GAO, Di DONG, Lei TANG, Xiaofang XING, Shuqin JIA, Ting GUO, Lianhai ZHANG, Fei SHAN, Xin JI, Anqiang WANG. Development and dissemination of precision medicine approaches in gastric cancer management [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 864-867. |
| [3] | Bowen LI, Qiang ZHANG, Yixin SUN. Establishment and validation of a risk prediction model for scoliosis after Nuss procedure in children and young adults with pectus excavatum [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 941-946. |
| [4] | Xiaoyong YANG, Fan ZHANG, Lulin MA, Cheng LIU. Clinical characteristics and influencing factors of extraglandular invasion of prostatic ductal adenocarcinoma [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 956-960. |
| [5] | Wanwei HUANG, Xianshen SHA, Yibao ZHANG, Guohao WU, Feng LUO, Zhihui CHEN, Dongming YE, Xuesong LI, Caiyong LAI. Total 3D laparoscopic ileal ureters replacement for bilateral ureters combined with bladder augmentation in the management of post-radiotherapy bilateral ureteral strictures and contracted bladder [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 789-795. |
| [6] | Yuanmei LIU, Yicheng FU, Jingxin HAO, Fuchun ZHANG, Huilin LIU. Construction and validation of a nomogram for predicting in-hospital postoperative heart failure in elderly patients with hip fracture [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 874-883. |
| [7] | Zhicun LI, Tianyu WU, Lei LIANG, Yu FAN, Yisen MENG, Qian ZHANG. Risk factors analysis and nomogram model construction of postoperative pathological upgrade of prostate cancer patients with single core positive biopsy [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 896-901. |
| [8] | Ye YAN,Xiaolong LI,Haizhui XIA,Xuehua ZHU,Yuting ZHANG,Fan ZHANG,Ke LIU,Cheng LIU,Lulin MA. Analysis of risk factors for long-term overactive bladder after radical prostatectomy [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 589-593. |
| [9] | Shuhui YU,Jianing HAN,Lijun ZHONG,Congyu CHEN,Yunxiang XIAO,Yanbo HUANG,Yang YANG,Xinyan CHE. Predictive value of preoperative pelvic floor electrophysiological parameters on early urinary incontinence following radical prostatectomy [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 594-599. |
| [10] | Zezhen ZHOU,Shaohui DENG,Ye YAN,Fan ZHANG,Yichang HAO,Liyuan GE,Hongxian ZHANG,Guoliang WANG,Shudong ZHANG. Predicting the 3-year tumor-specific survival in patients with T3a non-metastatic renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 673-679. |
| [11] | Junqi SU,Xiaoying WANG,Zhiqiang SUN. Establishment and verification of a prognostic nomogram for survival of tongue squamous cell carcinoma patients who underwent cervical dissection [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 120-130. |
| [12] | Zhan-yi ZHANG,Fan ZHANG,Ye YAN,Cai-guang CAO,Chang-jian LI,Shao-hui DENG,Yue-hao SUN,Tian-liang HUANG,Yun-he GUAN,Nan LI,Min LU,Zhen-hua HU,Shu-dong ZHANG. Near-infrared targeted probe designed for intraoperative imaging of prostatic neurovascular bundles [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 843-850. |
| [13] | ZHANG Fan,CHEN Qu,HAO Yi-chang,YAN Ye,LIU Cheng,HUANG Yi,MA Lu-lin. Relationship between recovery of urinary continence after laparoscopic radical prostatectomy and preoperative/postoperative membranous urethral length [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 299-303. |
| [14] | DING Ting-ting,ZENG Chu-xiong,HU Li-na,YU Ming-hua. Establishment of a prediction model for colorectal cancer immune cell infiltration based on the cancer genome atlas (TCGA) database [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 203-208. |
| [15] | HAO Han,LIU Yue,CHEN Yu-ke,SI Long-mei,ZHANG Meng,FAN Yu,ZHANG Zhong-yuan,TANG Qi,ZHANG Lei,WU Shi-liang,SONG Yi,LIN Jian,ZHAO Zheng,SHEN Cheng,YU Wei,HAN Wen-ke. Evaluating continence recovery time after robot-assisted radical prostatectomy [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 697-703. |
|
||