Journal of Peking University (Health Sciences) ›› 2023, Vol. 55 ›› Issue (6): 982-992. doi: 10.19723/j.issn.1671-167X.2023.06.005
Previous Articles Next Articles
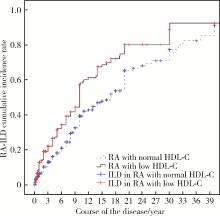
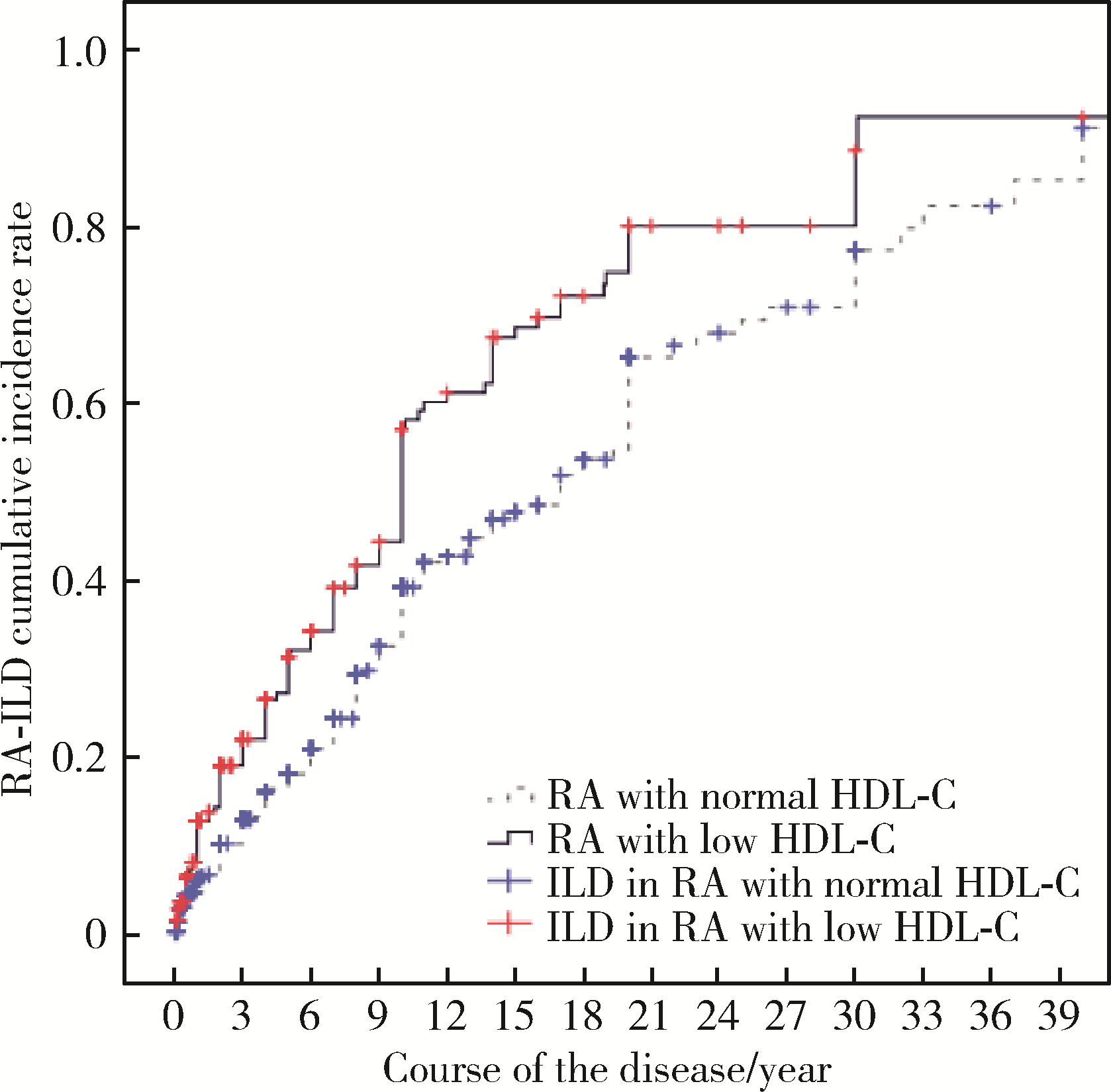
Correlation between dyslipidemia and rheumatoid arthritis associated interstitial lung disease
Qi WU1,2,Yue-ming CAI1,Juan HE1,Wen-di HUANG3,Qing-wen WANG1,*( )
)
- 1. Department of Rheumatism and Immunology, Peking University Shenzhen Hospital; Shenzhen Key Laboratory of Immunity and Inflammatory Diseases, Shenzhen 518000, Guangdong, China
2. Shantou University Medical College, Shantou 515000, Guangdong, China
3. Department of Pulmonary and Critical Care Medicine, Peking University Shenzhen Hospital Shenzhen, Shenzhen 518000, Guangdong, China
CLC Number:
- R593.2
| 1 |
Figus FA , Piga M , Azzolin I , et al. Rheumatoid arthritis: Extra-articular manifestations and comorbidities[J]. Autoimmun Rev, 2021, 20 (4): 102776.
doi: 10.1016/j.autrev.2021.102776 |
| 2 | Suda T . UP-to-date information on rheumatoid arthritis-associated interstitial lung disease[J]. Clin Med Insights Circ Respir Pulm Med, 2015, 9, 155- 162. |
| 3 |
Hyldgaard C , Hilberg O , Pedersen AB , et al. A population-based cohort study of rheumatoid arthritis-associated interstitial lung disease: Comorbidity and mortality[J]. Ann Rheum Dis, 2017, 76, 1700- 1706.
doi: 10.1136/annrheumdis-2017-211138 |
| 4 |
Fazeli M S , Khaychuk V , Wittstock K , et al. Rheumatoid arthritis-associated interstitial lung disease: Epidemiology, risk/prognostic factors, and treatment landscape[J]. Clin Exp Rheumatol, 2021, 39 (5): 1108- 1118.
doi: 10.55563/clinexprheumatol/h9tc57 |
| 5 | Uzma E , Tasnim A , Danish K . Lipid abnormalities in patients with rheumatoid arthritis[J]. Pak J Med SCI, 2017, 33 (1): 227- 230. |
| 6 | 陈哲. 血清脂蛋白异常与IPF关系及其临床意义[D]. 广西: 广西医科大学, 2018. |
| 7 |
Aletaha D , Neogi T , Silman AJ , et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative[J]. Arthritis Rheum, 2010, 62 (9): 2569- 2581.
doi: 10.1002/art.27584 |
| 8 |
Travis WD , Costabel U , Hansell DM , et al. An official American Thoracis Society/European Respiratory Society statement: Update of the international multisciplinary classification of the idiopathic interstitial pneumonias[J]. Am J Respir Crit Care Med, 2013, 188 (6): 733- 748.
doi: 10.1164/rccm.201308-1483ST |
| 9 | 中国成人血脂异常防治指南修订联合委员会. 中国成人血脂异常防治指南(2016年修订版)[J]. 中华全科医师杂志, 2017, 16 (1): 15- 35. |
| 10 |
Semb AG , Ikdahl E , Wibetoe G , et al. Atherosclerotic cardiovascular disease prevention in rheumatoid arthritis[J]. Nat Rev Rheumatol, 2020, 16 (7): 361- 379.
doi: 10.1038/s41584-020-0428-y |
| 11 |
Hollan I , Ronda N , Dessein P , et al. Lipd management in rheumatoid arthritis: A position paper of the Working Group on Cardiovascular Pharmacotherapy of the European Society of Cardiology[J]. Eur Heart J Cardiovasc Pharmacother, 2020, 6 (2): 104- 114.
doi: 10.1093/ehjcvp/pvz033 |
| 12 |
Charles-Schoeman C , Meriwether D , Lee YY , et al. High levels of oxidized fatty acids in HDL are associated with impaired HDL function in patients with active rheumatoid arthritis[J]. Clin Rheumatol, 2018, 37 (3): 615- 622.
doi: 10.1007/s10067-017-3896-y |
| 13 | Gordon EM , Figueroa DM , Barochia AV , et al. High-density lipoproteins and apolipoprotein A-I: Potential new players in the prevention and treatment of lung disease[J]. Front Pharmacol, 2016, 7, 323. |
| 14 |
Hee LE , Eun-Ju L , Jeong KH , et al. Overexpression of apolipoprotein A1 in the lung abrogates fibrosis in experimental silicosis[J]. PloS One, 2013, 8 (2): e55827.
doi: 10.1371/journal.pone.0055827 |
| 15 |
Belchamber K , Donnelly L E . Targeting defective pulmonary innate immunity: A new therapeutic option?[J]. Pharmacol Ther, 2020, 209, 107500.
doi: 10.1016/j.pharmthera.2020.107500 |
| 16 | Tall AR , Yvan-Charvet L . Cholesterol, inflammation and innate immunity[J]. Nat Rev Immunol, 2015, 15 (2): 104- 116. |
| 17 | Laurent YC , Fabrizia B , Renè GR , et al. Immunometabolic function of cholesterol in cardiovascular disease and beyond[J]. Cardiovasc Res, 2019, 115 (9): 1393- 1407. |
| 18 | Chistiakov DA , ORekhov AN , Bobryshev YV . ApoA1 and ApoA1-specific self-antibodies in cardiovascular disease[J]. Lab Invest, 2016, 96 (7): 708- 718. |
| 19 | Vuilleumier N , Bratt J , Alizadeh R , et al. Anti-apoA-1 IgG and oxidized LDL are raised in rheumatoid arthritis (RA): Potential associations with cardiovascular disease and RA disease activity[J]. Scand J Rheumatol, 2010, 39 (6): 447- 453. |
| 20 | Salaffi F , Carotti M , di Carlo M , et al. High-resolution computed tomography of the lung in patients with rheumatoid arthritis: Prevalence of interstitial lung disease involvement and determinants of abnormalities[J]. Medicine (Baltimore), 2019, 98 (38): e17088. |
| 21 | Kelly CA , Saravanan V , Nisar M , et al. Rheumatoid arthritis-related interstitial lung disease: associations, prognostic factors and physiological and radiological characteristics: A large multicentre UK study[J]. Rheumatology (Oxford), 2014, 53 (9): 1676- 1682. |
| 22 | Ito Y , Arita M , Kumagai S , et al. Radiological fibrosis score is strongly associated with worse survival in rheumatoid arthritis-related interstitial lung disease[J]. Mod Rheumatol, 2019, 29 (1): 98- 104. |
| [1] | Doudou ZHAO, Xuan QI, Bo HUANG, Weibo GAO, Yuanyuan PEI, Yuebo JIN, Miao SHAO, Jing HE. Expression and clinical significance of lymphocyte subsets in infectious pneumonia and immune-related interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 624-630. |
| [2] | Hui WEI, Jingfeng ZHANG, Zhongqiang YAO, Jinxia ZHAO. Clinical characteristics and relevant factors of rheumatoid arthritis patients with anemia of chronic disease [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 307-312. |
| [3] | Tao WU, Jianzi LIN, Yafeng ZHU, Jianda MA, Peiwen JIA, Lijuan YANG, jie PAN, Yaowei ZOU, Ying YANG, Ye LU, Lie DAI. Serum inter-alpha-trypsin inhibitor heavy chain H3 is identified as a potential biomarker for myopenia in patients with rheumatoid arthritis using proteomic profiling [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1024-1031. |
| [4] | Jingwen LAN, Zhe CHEN, Yongjing CHENG, Like ZHAO. Clinical characteristics, efficacy and safety of antifibrotic agents in elderly patients with connective tissue disease-associated interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1101-1106. |
| [5] | Yan DING, Lifang WANG, Chaoran LI, Zhemin LU, Lianjie SHI. Rheumatoid arthritis combined with IgG4-related disease successfully treated with rituximab: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1203-1207. |
| [6] | Ju YANG, Jing XU, Juhua DAI, Lianjie SHI. Expression of lumican protein in serum of patients with rheumatoid arthritis and its correlation with disease and immune activities [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 911-918. |
| [7] | Lianghua FENG, Lirong HONG, Yujia CHEN, Xueming CAI. Role and mechanism of ubiquitin-specific protease 35 in ferroptosis of rheumatoid arthritis-fibroblast like synoviocytes [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 919-925. |
| [8] | Peiwen JIA, Ying YANG, Yaowei ZOU, Zhiming OUYANG, Jianzi LIN, Jianda MA, Kuimin YANG, Lie DAI. Clinical characteristics of overlapping syndromes of low muscle mass in patients with rheumatoid arthritis and their impact on physical function [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1009-1016. |
| [9] | Doudou MA, Zhemin LU, Qian GUO, Sha ZHU, Jin GU, Yan DING, Lianjie SHI. Successful treatment of rheumatoid arthritis complicated with myasthenia gravis with low-dose rituximab: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1110-1114. |
| [10] | Rui YAN, Dan KE, Yan ZHANG, Li LI, Huanran SU, Wei CHEN, Mingxia SUN, Xiaomin LIU, Liang LUO. Diagnostic significance of serum chemokine CXCL-10 and Krebs von den lungen-6 level in patients with rheumatoid arthritis associated interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 956-962. |
| [11] | Liang ZHAO, Chenglong SHI, Ke MA, Jing ZHAO, Xiao WANG, Xiaoyan XING, Wanxing MO, Yirui LIAN, Chao GAO, Yuhui LI. Immunological characteristics of patients with anti-synthetase syndrome overlap with rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 972-979. |
| [12] | Yujing ZHU, Lei WANG, Chengyin LYU, Wenfeng TAN, Miaojia ZHANG. Analysis of clinical features of ruccrent interstitial lung disease in patients with anti-EJ positive antisynthetase syndrome [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 980-986. |
| [13] | Yijun HAN, Xiaoli CHEN, Changhong LI, Jinxia ZHAO. Application status of methotrexate in patients with rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 994-1000. |
| [14] | Dongwu LIU, Jie CHEN, Mingli GAO, Jing YU. Rheumatoid arthritis with Castleman-like histopathology in lymph nodes: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 928-931. |
| [15] | Huina HUANG,Jing ZHAO,Xiangge ZHAO,Ziran BAI,Xia LI,Guan WANG. Regulatory effect of lactate on peripheral blood CD4+ T cell subsets in patients with rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 519-525. |
|
||