Journal of Peking University (Health Sciences) ›› 2024, Vol. 56 ›› Issue (6): 980-986. doi: 10.19723/j.issn.1671-167X.2024.06.006
Previous Articles Next Articles
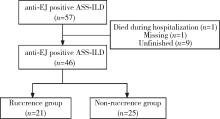
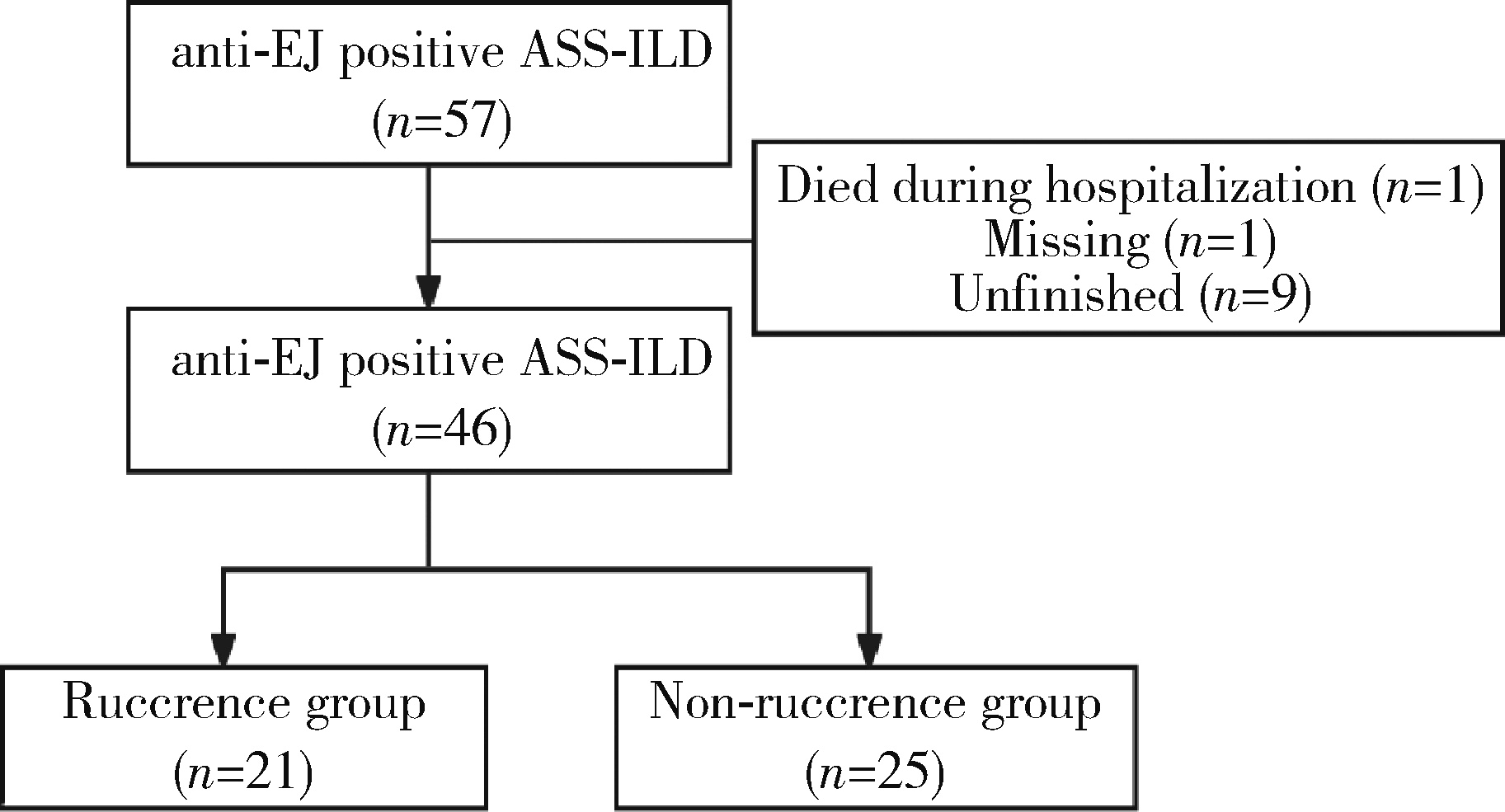
Analysis of clinical features of ruccrent interstitial lung disease in patients with anti-EJ positive antisynthetase syndrome
Yujing ZHU, Lei WANG, Chengyin LYU, Wenfeng TAN, Miaojia ZHANG*( )
)
- Department of Rheumatology and Immunology, the First Affiliated Hospital of Nanjing Medical University, Nanjing 210029, China
CLC Number:
- R563
| 1 |
Aggarwal R , Cassidy E , Fertig N , et al. Patients with non-Jo-1 anti-tRNA synthetase autoantibodies have worse survival than Jo-1 positive patients[J]. Ann Rheum Dis, 2014, 73 (1): 227- 232.
doi: 10.1136/annrheumdis-2012-201800 |
| 2 | Sreevilasan SK , Devarasetti P , Narahari NK , et al. Clinical profile and treatment outcomes in antisynthetase syndrome: A tertiary centre experience[J]. Rheumatol Adv Pract, 2021, 5 (Suppl 2): ii10- ii18. |
| 3 |
Hamaguchi Y , Fujimoto M , Matsushita T , et al. Common and distinct clinical features in adult patients with anti-aminoacyl-tRNA synthetase antibodies: Heterogeneity within the syndrome[J]. PLoS One, 2013, 8 (4): e60442.
doi: 10.1371/journal.pone.0060442 |
| 4 |
Teel A , Lu J , Park J , et al. The role of myositis-specific autoantibodies and the management of interstitial lung disease in idiopathic inflammatory myopathies: A systematic review[J]. Semin Arthritis Rheum, 2022, 57, 152088.
doi: 10.1016/j.semarthrit.2022.152088 |
| 5 |
Zhang Y , Ge Y , Yang H , et al. Clinical features and outcomes of the patients with anti-glycyl tRNA synthetase syndrome[J]. Clin Rheumatol, 2020, 39 (8): 2417- 2424.
doi: 10.1007/s10067-020-04979-8 |
| 6 |
Watanabe K , Handa T , Tanizawa K , et al. Detection of antisynthetase syndrome in patients with idiopathic interstitial pneumonias[J]. Respir Med, 2011, 105 (8): 1238- 1247.
doi: 10.1016/j.rmed.2011.03.022 |
| 7 |
Sasano H , Hagiwara E , Kitamura H , et al. Long-term clinical course of anti-glycyl tRNA synthetase (anti-EJ) antibody-related interstitial lung disease pathologically proven by surgical lung biopsy[J]. BMC Pulm Med, 2016, 16 (1): 168.
doi: 10.1186/s12890-016-0325-y |
| 8 |
Hozumi H , Fujisawa T , Nakashima R , et al. Efficacy of glucocorticoids and calcineurin inhibitors for anti-aminoacyl-trna synthetase antibody-positive polymyositis/dermatomyositis-associated interstitial lung disease: A propensity score-matched analysis[J]. J Rheumatol, 2019, 46 (5): 509- 517.
doi: 10.3899/jrheum.180778 |
| 9 | Yorishima Y , Tominaga M , Fujimoto K , et al. Combination of prednisolone and calcineurin inhibitors prevents lung function decline in patients with anti-aminoacyl-tRNA synthetase antibody-positive polymyositis/dermatomyositis[J]. Kurume Med J, 2023, 69 (1/2): 19- 30. |
| 10 |
Martínez-García EA , Lujano-Benítez AV , Gercía-De La Torre Ⅰ , et al. Good response to mycophenolate mofetil on treatment of interstitial lung disease in polymyositis associated with antisynthetase syndrome positive for anti-EJ and anti-Ro52 antibodies[J]. Clin Rheumatol, 2020, 39 (9): 2837- 2839.
doi: 10.1007/s10067-020-05075-7 |
| 11 |
Langlois V , Gillibert A , Uzunhan Y , et al. Rituximab and cyclophosphamide in antisynthetase syndrome-related interstitial lung disease: An observational retrospective study[J]. J Rheumatol, 2020, 47 (11): 1678- 1686.
doi: 10.3899/jrheum.190505 |
| 12 |
Liu Y , Liu X , Xie M , et al. Clinical characteristics of patients with anti-EJ antisynthetase syndrome associated interstitial lung disease and literature review[J]. Respir Med, 2020, 165, 105920.
doi: 10.1016/j.rmed.2020.105920 |
| 13 |
Connors GR , Christopher-Stine L , Oddis CV , et al. Interstitial lung disease associated with the idiopathic inflammatory myopathies: What progress has been made in thepast 35 years[J]. Chest, 2010, 138 (6): 1464- 1474.
doi: 10.1378/chest.10-0180 |
| 14 |
Bohan A , Peter JB . Polymyositis and dermatomyositis (first of two parts)[J]. N Engl J Med, 1975, 292 (7): 344- 347.
doi: 10.1056/NEJM197502132920706 |
| 15 |
Raghu G , Remy-Jardin M , Richeldi L , et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: An official ATS/ERS/JRS /ALAT clinical practice guideline[J]. Am J Respir Crit Care Med, 2022, 205 (9): e18- e47.
doi: 10.1164/rccm.202202-0399ST |
| 16 |
Targoff IN . Autoantibodies to aminoacyl-transfer RNA synthetases for isoleucine and glycine. Two additional synthetases are antigenic in myositis[J]. J Immunol, 1990, 144 (5): 1737- 1743.
doi: 10.4049/jimmunol.144.5.1737 |
| 17 | Tang HS, Tang IYK, Ho RTC, et al. Clinical heterogeneity and prognostic factors of anti-synthetase syndrome: A multi-centered retrospective cohort study[J]. Rheumatology (Oxford), 2023 (2023-12-14)[2024-09-01]. https://Doi.org/10.1093/rheumatology/kead671. |
| 18 |
García-Bravo L , Calle-Rubio M , Fernández-Arquero M , et al. Association of anti-SARS-COV-2 vaccine with increased incidence of myositis-related anti-RNA-synthetases auto-antibodies[J]. J Transl Autoimmun, 2022, 5, 100160.
doi: 10.1016/j.jtauto.2022.100160 |
| 19 | Irie Y , Wakabayashi H , Matuzawa Y , et al. A case of anti-synthetase syndrome with anti-glycyl tRNA synthetases antibody de-veloped after COVID-19[J]. Cureus, 2024, 16 (4): e58004. |
| 20 |
Shimizu H , Matsumoto H , Sasajima T , et al. New-onset dermatomyositis following COVID-19: A case report[J]. Front Immunol, 2022, 13, 1002329.
doi: 10.3389/fimmu.2022.1002329 |
| 21 | Peña C , Kalara N , Velagapudi P . A case of antisynthetase syndrome in the setting of SARS-Cov-2 infection[J]. Cureus, 2023, 15 (6): e40588. |
| 22 |
Elsayed M , Abdelgabar A , Karmani J , et al. A case of antisynthetase syndrome initially presented with interstitial lung disease mimicking COVID-19[J]. J Med Cases, 2023, 14 (1): 25- 30.
doi: 10.14740/jmc4031 |
| 23 | Tranah E , MacBrayne A , Bhadauria N , et al. A case of antisynthetase syndrome presenting solely with life-threatening interstitial lung disease[J]. Clin Med (Lond), 2023, 23 (1): 85- 87. |
| 24 | 周云, 吕成银, 尤含笑, 等. 不同抗体亚型抗合成酶综合征并发间质性肺疾病临床特征分析[J]. 中华风湿病学杂志, 2024, 28 (8): 538- 544. |
| [1] | Doudou ZHAO, Xuan QI, Bo HUANG, Weibo GAO, Yuanyuan PEI, Yuebo JIN, Miao SHAO, Jing HE. Expression and clinical significance of lymphocyte subsets in infectious pneumonia and immune-related interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 624-630. |
| [2] | Jingwen LAN, Zhe CHEN, Yongjing CHENG, Like ZHAO. Clinical characteristics, efficacy and safety of antifibrotic agents in elderly patients with connective tissue disease-associated interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1101-1106. |
| [3] | Fengyi HU, Qingyang MENG, Nayun CHEN, Jianing WANG, Zhenlong LIU, Yong MA, Yuping YANG, Xi GONG, Cheng WANG, Ping LIU, Weili SHI. Clinical efficacy of arthroscopic medial patellofemoral complex reconstruction for recurrent patellar dislocation with high-grade trochlear dysplasia [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 947-955. |
| [4] | Yukai LI, Hongyan WANG, Liang LUO, Yun LI, Chun LI. Clinical significance of antiphospholipid antibodies in Behcet disease with thrombosis [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1036-1040. |
| [5] | Rui YAN, Dan KE, Yan ZHANG, Li LI, Huanran SU, Wei CHEN, Mingxia SUN, Xiaomin LIU, Liang LUO. Diagnostic significance of serum chemokine CXCL-10 and Krebs von den lungen-6 level in patients with rheumatoid arthritis associated interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 956-962. |
| [6] | Yuqing LI,Biao WANG,Peng QIAO,Wei WANG,Xing GUAN. Medium to long-term efficacy of tension-free vaginal tape procedure in the treatment of female recurrent stress urinary incontinence [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 600-604. |
| [7] | Zhanhong LAI,Jiachen LI,Zelin YUN,Yonggang ZHANG,Hao ZHANG,Xiaoyan XING,Miao SHAO,Yuebo JIN,Naidi WANG,Yimin LI,Yuhui LI,Zhanguo LI. A unicenter real-world study of the correlation factors for complete clinical response in idiopathic inflammatory myopathies [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 284-292. |
| [8] | Qi WU,Yue-ming CAI,Juan HE,Wen-di HUANG,Qing-wen WANG. Correlation between dyslipidemia and rheumatoid arthritis associated interstitial lung disease [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 982-992. |
| [9] | Wen-gen LI,Xiao-dong GU,Rui-qiang WENG,Su-dong LIU,Chao CHEN. Expression and clinical significance of plasma exosomal miR-34-5p and miR-142-3p in systemic sclerosis [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1022-1027. |
| [10] | Chieko MORIMOTO,Yi-qin WANG,Rong ZHOU,Jian-liu WANG. Clinical analysis of fertility-sparing therapy of patients with complex atypical hyperplasia and endometrial cancer [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 936-942. |
| [11] | Yue WANG,Shuang ZHANG,Hong ZHANG,Li LIANG,Ling XU,Yuan-jia CHENG,Xue-ning DUAN,Yin-hua LIU,Ting LI. Clinicopathological features and prognosis of hormone receptor-positive/human epidermal growth factor receptor 2-negative breast cancer [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 853-862. |
| [12] | Su-hua CHEN,Jun YANG,Xin CHEN,Chen-long YANG,Jian-jun SUN,Guo-zhong LIN,Tao YU,Xin YANG,Yun-feng HAN,Chao WU,Yu SI,Kai-ming MA. Surgical treatment of large and giant recurrent meningiomas near the middle and posterior third part of the superior sagittal sinus with extracranial invading [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 1006-1012. |
| [13] | ZHANG Pu-li,YANG Hong-xia,ZHANG Li-ning,GE Yong-peng,PENG Qing-lin,WANG Guo-chun,LU Xin. Value of serum YKL-40 in the diagnosis of anti-MDA5-positive patients with dermatomyositis complicated with severe pulmonary injury [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1055-1060. |
| [14] | LIU Lei,QIN Yan-chun,WANG Guo-liang,ZHANG Shu-dong,HOU Xiao-fei,MA Lu-lin. Strategy of reoperation for pheochromocytoma and paraganglioma [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 793-797. |
| [15] | XIA Fang-fang,LU Fu-ai,LV Hui-min,YANG Guo-an,LIU Yuan. Clinical characteristics and related factors of systemic lupus erythematosus with interstitial pneumonia [J]. Journal of Peking University (Health Sciences), 2021, 53(2): 266-272. |
|
||