
牙骨质-骨结构不良(cemento-osseous dysplasia,COD)属于临床少见的一种纤维-骨肿瘤及结构不良,好发于非洲人和东亚人,中年女性发病率较高[1]。一般无症状,常在X线检查时意外发现,其典型影像学表现与常见的牙髓源性的慢性根尖周炎相似,易误诊误治。部分患者可表现为颌骨膨隆,病灶区伴有感染时,可出现疼痛、溢脓等炎症性反应。本文报道1例就诊于北京大学国际医院口腔科的繁茂型牙骨质-骨结构不良(florid cemento-osseous dysplasia, FLCOD)患者,并对相关文献进行回顾。
1 病例临床资料
患者女性,45岁,因“左下后牙充填体脱落3周”就诊,无冷热痛、自发痛、咬合痛、牙龈肿痛史。患者10年前行左下后牙治疗,1年前牙冠劈裂后行充填治疗。全身情况:患者有卵巢功能减退,现服用坤泰胶囊及地屈孕酮治疗。
临床检查:左右颌面部基本对称,无颌骨膨隆,面部及颌下未触及肿大淋巴结。咬合检查:前牙反牙合,无咬合早接触及咬合干扰。口腔卫生状况一般,牙石(+ +),软垢少量,探诊深度(probing depth,PD) 3~5 mm,附着丧失0~2 mm。
左下第一磨牙(36)咬合面大面积牙色充填体部分脱落,继发龋坏达髓腔,叩痛(-),不松动,牙龈未见窦道口,PD 3~4 mm。左下第二磨牙(37)烤瓷冠,边缘密合。左下及右下第三磨牙(38、48)牙冠完整。右下第一及第二磨牙(46、47) 牙合面牙色充填体,边缘无龋坏。牙髓电活力测试结果为 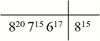 。
。
。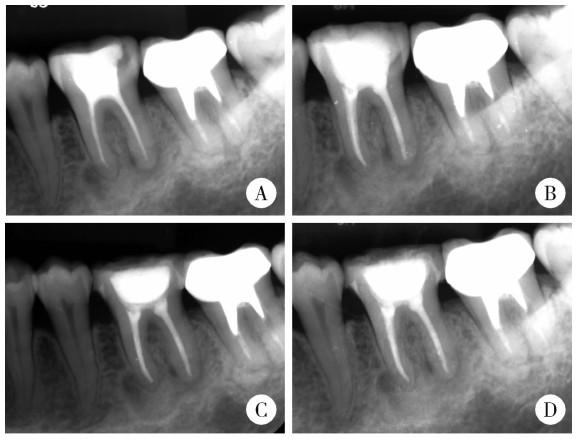
图1 左下颌第一磨牙(36)的术前和术后根尖片Figure 1 Preoperative and postoperative periapical radiographs of the mandibular left first molar (36) A, preoperative periapical radiolucency showing well-defined radiopaque mass with radiolucent border; B, postoperative radiograph of completed root filling; C and D, 3-month and 6-month follow-up X-ray. |
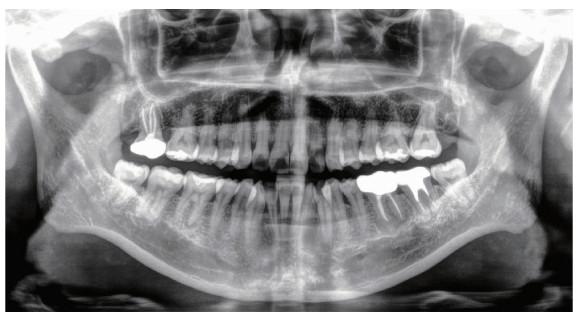
图2 患者初诊时的CBCT图像Figure 2 CBCT images of the patient at initial presentation Three radiographic stages of COD concurrently shown in multifocal lesions across six mandibular molars: osteolytic stage (38/46/48), cementoblastic stage (36/37), mature stage (47). The red arrow indicates the COD lesion. COD, cemento-osseous dysplasia; CBCT, cone beam computed tomographic. |
诊断:36继发龋(牙髓治疗后);繁茂型牙骨质-骨结构不良;慢性牙周炎。
治疗计划:36根管再治疗后全冠修复;牙骨质-骨结构不良病损每年定期检查;牙周洁治、刮治。
治疗过程:36根管再治疗后即刻行临时冠修复;牙周洁治、刮治。

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
36术后3个月、6个月、1年随访,患者无症状,拍摄根尖片示根尖周影像无明显变化,混合密度影大小约为11 mm×7 mm(图 1)。36术后1年去除临时冠,完成全冠修复。
2 讨论
2.1 诊断与鉴别诊断
患者为中年女性,主诉左下后牙充填体脱落,患牙有多次治疗史,无明显不适症状。因根尖片显示患牙根尖周存在大面积类圆形密度不均匀区域,为进一步评估该骨病损的影像学特征,行CBCT检查,显示患者双侧下颌后牙区多颗磨牙根尖周异常表现,最终诊断为FLCOD。诊断依据包括:患者无临床症状的病史,多象限累及牙的牙髓活髓状态,以及三维影像学呈现的多灶性混合密度病变特征。结合1年随访中病变稳定,符合世界卫生组织(World Health Organization,WHO)制定的FLCOD诊断标准[2]。本例的罕见性体现在其影像学呈现了骨质溶解破坏期、类牙骨质小体形成期与钙化成熟期三期并存的特点,为理解COD的自然进展提供了实例,且患者合并的卵巢功能减退提示了全身因素与颌骨病变的潜在关联。
鉴别诊断时,对于此类无症状、仅在影像学检查中偶然发现的COD病例,与慢性根尖周炎的区分尤为重要。由于两者在根尖片上均可表现为根周低密度影,临床上极易误诊,进而导致不必要的牙髓治疗。本病例支持FLCOD诊断的关键依据在于,多颗累及牙的牙髓活力测试反应正常,而慢性根尖周炎患牙通常伴随牙髓感染症状;影像学上,FLCOD病变内部可见高密度钙化团块,呈典型的混合密度特征,而非慢性根尖周炎常见的均匀透射影。另外,还需与牙骨质-骨化纤维瘤(cemento-ossifying fibroma, COsF)、家族性巨大型牙骨质瘤(familial gigantiform cementoma, FGC)及成牙骨质细胞瘤等影像学表现相似的疾病相鉴别[3-4]。本例病变未见明显膨胀性改变及骨皮质受累,不符合COsF作为真性肿瘤性病变多呈膨胀性生长伴骨皮质变薄的典型特征,故不支持COsF诊断。FGC虽也可表现为多象限混合密度影,但通常早期即出现颌骨膨大,本例患者无颌骨形态改变,可予以鉴别。本例患者受累牙的牙根完整、牙髓活力正常,不符合成牙骨质细胞瘤的典型特征,即牙根融合和牙根吸收。
2.2 治疗策略与预后分析
针对本病例病变状况及受累牙差异制定治疗计划,并积极控制患者局部及全身风险因素[9],颌骨FLCOD病变本身暂不予干预。多项回顾性研究表明,对于无症状且无影像学进展迹象的COD,手术干预非但无益,还可能因破坏病变周围血供而显著增加继发感染、伤口不愈合和病理性骨折的风险[10-12]。为控制潜在风险,我们针对患者局部因素,对慢性牙周炎实施了完善的牙周基础治疗以减轻牙周组织炎性刺激。在全身因素管理方面,以往研究表明,雌激素水平下降可破坏成骨与破骨细胞间的平衡,导致骨吸收大于骨形成[13]。雌激素治疗也被证实可促进牙槽骨新生、减少破骨细胞并提升骨保护素水平[14]。我们推测本例患者卵巢功能减退可能通过影响全身骨代谢,为颌骨局部异常骨与牙骨质沉积创造了有利的病理微环境,目前,患者规律接受坤泰胶囊及地屈孕酮药物治疗以维持骨代谢稳态。此外,患者存在反牙合问题,但临床检查未发现明确的咬合创伤体征,且患者无正畸治疗意愿,当前的处理策略为定期行咬合检查。针对受累牙,36因继发龋深达髓腔引发冠方微渗漏,且根尖周COD病灶的血供不足易发骨髓炎,故行根管再治疗控制感染,并行全冠修复预防牙齿劈裂,避免拔牙所致COD病变愈合不良风险;37牙根管充填完善且无症状,予观察随访;其余活髓牙(38、46、47、48)无牙体疾病,定期监测。
根据病变发展中血管化程度、纤维化进展及钙化沉积量的动态变化,COD在病理与影像学上可分为三期(表 1)。本例患者病变累及的6颗牙齿(36、37、38、46、47、48)根尖周影像学表现多样,同时呈现骨质溶解破坏期、类牙骨质小体形成期与钙化成熟期三期并存的特征,例如,38、46、48根尖周可见类圆形的低密度影,边缘伴硬化带,符合骨质溶解破坏期特点;36、37处于类牙骨质小体形成期,其根尖周低密度影内可见边界清晰的点状或团块状高密度影;47表现为钙化成熟期特征,均匀高密度团块影伴薄层透射边缘。
表1 牙骨质-骨结构不良三个分期的病理学和影像学表现Table 1 Pathological and radiographic features of the three stages of cemento-osseous dysplasia |
| Disease stage | Pathological manifestations | Radiographic manifestations |
| Osteolytic stage | Replacement of normal bone by cellular fibrous tissue without calcification | Well-demarcated periapical radiolucency with sclerotic borders |
| Cementoblastic stage | Progressive deposition of cementum-like droplets and woven bone within the fibrous stroma | Punctate or flocculent radiopacities within a radiolucent halo |
| Mature stage | Densely mineralized masses with peripheral fibrous encapsulation | Homogeneous radiopacities bordered by thin radiolucent rims |
患者当前病变整体处于稳定阶段,随访期间未见颌骨膨大或影像学进展。值得注意的是,仅47达到钙化成熟期,此期因形成致密无血管的牙骨质样组织而需警惕继发骨髓炎风险,如Sarmento等[15]报道的FLCOD病例,感染发生于以成熟钙化为主的病变中;其余受累牙病变仍处于骨质溶解破坏期或类牙骨质小体形成期,具有潜在继续发展的生物学活性;此外,未累及牙亦存在新发病变风险。对患者的预后评估需警惕颌骨膨大、牙齿移位或继发感染等提示病变活动的征象,一旦出现需考虑手术干预。本例患者同时存在卵巢功能减退,可能通过影响骨代谢状态为病变创造了有利的病理微环境,因此建议长期随访监测,每年通过临床及影像学检查评估病变动态变化。
2.3 COD的命名与分型
COD的首次确切描述可追溯至1956年[16],当时被称为“根尖周骨发育不良(periapical osseous dysplasia)”。由于人们对其组织来源及病理演变的认识不足,该疾病的分类在较长时间内存在争议。2017年,WHO头颈部肿瘤分类采纳了“牙骨质-骨结构不良(cemento-osseous dysplasia)”这一命名[17],涵盖此类具有特征性病理学及影像学表现的疾病,并依据发病部位与影像学特征将其分为三型:局灶型牙骨质-骨结构不良(focal cemento-osseous dysplasia, FocCOD)、根尖周型牙骨质-骨结构不良(periapical cemento-osseous dysplasia, PCOD)及FLCOD。2022年,更新的WHO分类[2]进一步细化了分型体系,新增了家族性繁茂型牙骨质-骨结构不良(fami-lial florid cemento-osseous dysplasia,FFCOD)作为第四种亚型。COD各亚型的临床表现各异,局灶型多为单发,以下颌后牙区最常见;根尖周型主要累及下颌前牙区,多个病灶可相互融合;繁茂型在颌骨中呈多灶性分布,常对称发生,甚至累及四个象限,可伴有颌骨轻度膨隆;家族性繁茂型呈常染色体显性遗传,无性别或种族倾向性,其特点为发病年龄早,常阻碍牙齿萌出及显著颌骨膨隆,影像学呈现典型FLCOD特征。
本例患者为临床少见的FLCOD病例,诊断主要依据其无临床症状的病程、牙髓状态及典型的影像学表现。治疗策略上,着重处理继发龋等伴发病变,控制局部与全身风险因素,而非针对COD病变本身进行干预,预后还需长期随访。本病例的诊疗提示,口腔临床医师应加强对COD的识别与诊断能力,避免误诊和过度治疗。