
1 资料与方法
1.1 临床资料
1.2 活体组织取材
1.3 DIF检测
1.4 ELISA检测
1.5 统计学方法
2 结果
2.1 临床资料
2.2 组织病理特征
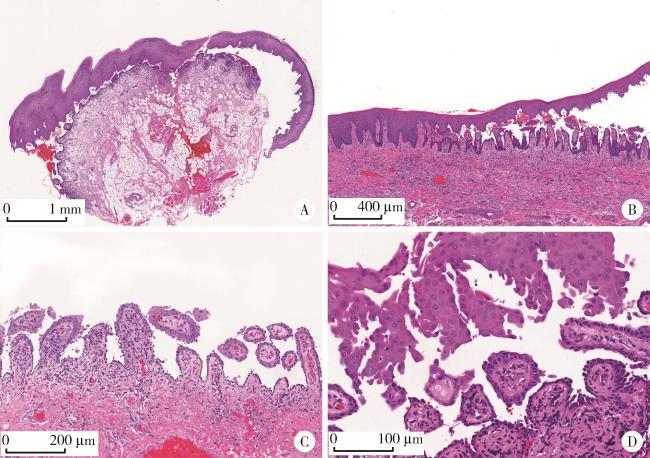
图1 口腔黏膜寻常型天疱疮的组织病理学特征(HE染色)Figure 1 Histopathological features of oral mucosal pemphigus vulgaris (HE staining) A, intraepithelial blister formation (×20); B, acantholysis (×40); C, blister roof detachment, with epithelial basal cells attached to the surface of connective tissue papillae showing a villous appearance (×100); D, acantholysis with scattered Tzanck cells: swollen round cells with hyperchromatic nuclei, often surrounded by a perinuclear cytoplasmic halo (×200). HE, hematoxylin-eosin. |
2.3 DIF检测结果
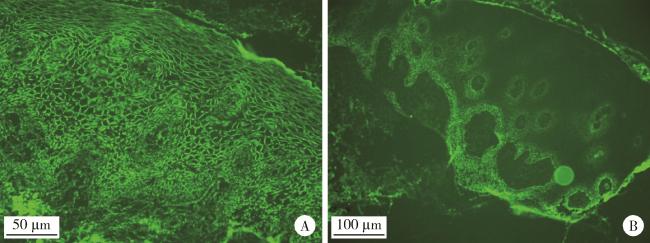
图2 口腔黏膜寻常型天疱疮的直接免疫荧光表现Figure 2 Direct immunofluorescence of oral mucosal pemphigus vulgaris A, a reticular pattern of IgG deposition is observed in the intercellular spaces of the epithelial stratum spinosum (excitation wavelength 488 nm, emission wavelength 520-530 nm, ×400); B, a reticular pattern of C3 deposition is observed in the intercellular spaces of the epithelial stratum spinosum (excitation wavelength 488 nm, emission wavelength 520-530 nm, ×200). |
表1 2例直接免疫荧光结果阴性患者的诊断及治疗情况Table 1 Diagnosis and treatment status of 2 patients with negative direct immunofluorescence results |
| Patient | Diagnosis | Treatment | |||||
| Clinical manifestation | Histopathology | Antibody level by ELISA/(U/mL) | Treated with pemphigus protocol | Used glucocorticoids | Treatment outcome | ||
| No.1 | Typical | Atypical | Anti-Dsg3: 93.70 (>20) Anti-Dsg1: 0 (< 20) | Yes | Yes | Marked | |
| No.2 | Typical | Atypical | Anti-Dsg3: 58.44 (>20) Anti-Dsg1: 11.33 (< 20) | Yes | No | Mild | |
ELISA, enzyme-linked immunosorbnent assay. |
2.4 ELISA检测结果
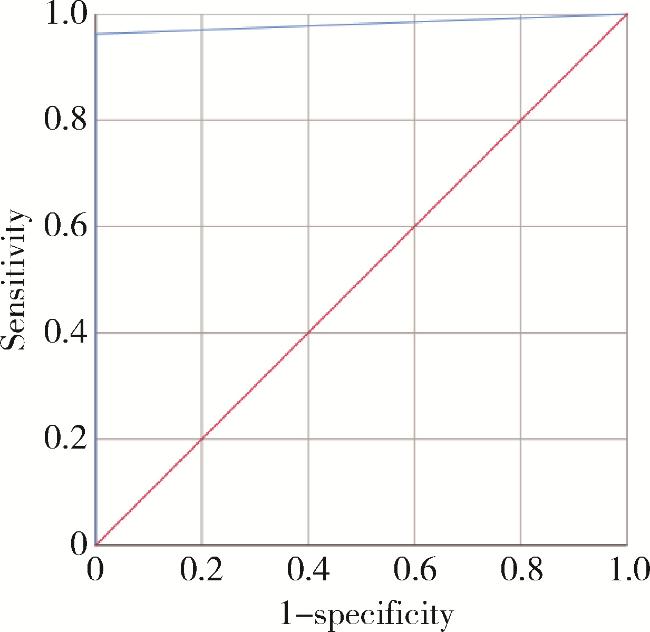
2.5 DIF的诊断效能评估
表2 直接免疫荧光各抗体指标的诊断效能Table 2 Diagnostic performance of various direct immunofluorescence antibody indicators |
| Detection indicator | Sensitivity | Specificity | Positive predictive value | Negative predictive value | Missed diagnosis rate | False positive rate |
| IgG | 92.45% | 55.00% | 84.48% | 73.33% | 7.55% | 45.00% |
| C3 | 52.83% | 60.00% | 77.78% | 32.43% | 47.17% | 40.00% |
| Fibrinogen | 20.75% | 75.00% | 68.75% | 26.32% | 79.25% | 25.00% |
| IgA | 5.66% | 85.00% | 50.00% | 25.37% | 94.34% | 15.00% |
| IgM | 1.89% | 95.00% | 50.00% | 26.76% | 98.11% | 5.00% |
| DIF | 96.23% | 100.00% | 100.00% | 90.91% | 3.77% | 0.00% |
Ig, immunoglobulin; C3, complement 3; DIF, direct immunofluorescence. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
2.6 不同检测方法诊断效能的比较
表3 口腔黏膜天疱疮中不同检测方法诊断效能的比较Table 3 Comparison of diagnostic performance of different detection methods in oral mucosal pemphigus vulgaris |
| Detection method | Sensitivity | Specificity | AUC |
| DIF | 96.23% | 100.00% | 0.981 |
| Histopathology | 94.34% | 100.00% | 0.972 |
| ELISA | 82.61% | 82.35% | 0.825 |
| Clinical diagnosis | 86.79% | 15.00% | 0.509 |
DIF, direct immunofluorescence; ELISA, enzyme-linked immunosorbnent assay; AUC, area under curve. |