北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (5): 883-890. doi: 10.19723/j.issn.1671-167X.2021.05.012
固定袢和可调节袢在粗骨道中的长度对股骨骨道增宽及膝关节功能的影响
印钰,梅宇,王泽刚,宋首一,刘鹏飞,何鹏峰,武文杰( ),谢兴()
),谢兴()
- 北京大学第三医院运动医学科,北京大学运动医学研究所,运动医学关节伤病北京市重点实验室,北京 100191
Lengths of the fixed loop and the adjustable loop in the coarse bone tunnel were compared to influence the widening of the femoral bone tunnel and the function of the knee joint
YIN Yu,MEI Yu,WANG Ze-gang,SONG Shou-yi,LIU Peng-fei,HE Peng-feng,WU Wen-jie(),XIE Xing()
- Beijing Key Laboratory of Sports Injuries, Beijing 100191, China
摘要:
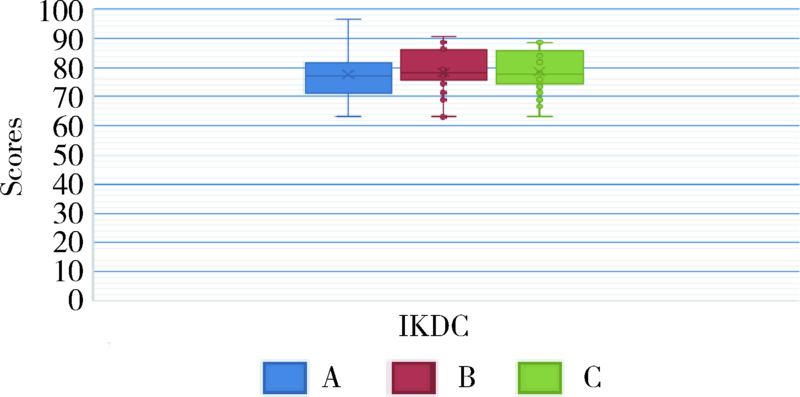
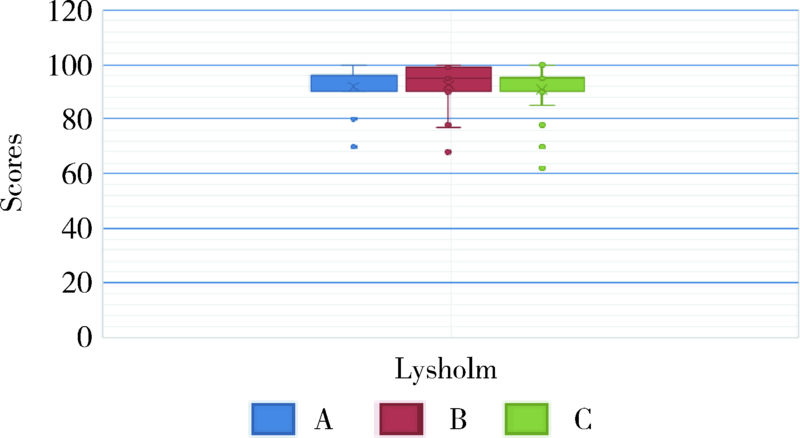
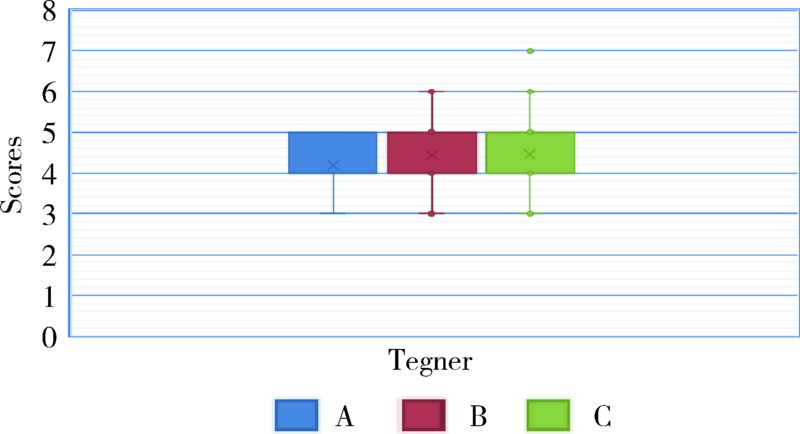
目的: 评估两种不同的股骨皮质悬吊装置(固定袢和可调节袢)重建前交叉韧带术后12个月患者的股骨骨道增宽情况及膝关节功能。方法: 共纳入60例行前交叉韧带重建术的患者,根据袢在粗骨道中长度(n)[n=袢的总长度-(股骨骨道总长度-粗骨道的总长度)]将患者分为A(可调节袢在粗骨道中长度为0 mm)、B(固定袢在粗骨道中长度为>0 mm、≤10 mm之间)、C(固定袢在粗骨道中长度>10 mm)三组,其中A组病例数为11例,B组病例数为27例,C组病例数为22例,比较三组患者在膝CT关节三维重建术后12个月与术后即刻股骨骨道增宽情况,同时比较三组患者的国际膝关节委员会(International Knee Documentation Committee,IKDC)评分、Lysholm评分及Tegner评分。结果: A、B、C三组的股骨骨道增宽程度存在差异,术后12个月和术后即刻股骨骨道增宽差值中位数:A
中图分类号:
- R686.5





| [1] |
Saccomanno MF, Shin JJ, Mascarenhas R, et al. Clinical and functional outcomes after anterior cruciate ligament reconstruction using cortical button fifixation versus transfemoral suspensory fixation: A systematic review of randomized controlled trials [J]. Arthroscopy, 2014, 30(11):1491-1498.
doi: 10.1016/j.arthro.2014.05.028 |
| [2] |
Han DL, Nyland J, Kendzior M, et al. Intratunnel versus extratunnel fixation of hamstring autograft for anterior cruciate ligament reconstruction [J]. Arthroscopy, 2012, 28(12):1555-1566.
doi: 10.1016/j.arthro.2012.02.021 |
| [3] |
Jansson KA, Harilainen A, Sandelin J, et al. Bone tunnel enlargement after anterior cruciate ligament reconstruction with the hamstring autograft and endobutton fifixation technique A clinical, radiographic and magnetic resonance imaging study with 2 years follow-up [J]. Knee Surg Sports Traumatol Arthroscopy, 1999, 7(5):290-295.
doi: 10.1007/s001670050166 |
| [4] |
Choi NH, Yang BS, Victoroff BN. Clinical and radiological outcomes after hamstring anterior cruciate ligament reconstructions: Comparison between fifixed-loop and adjustable-loop cortical suspension devices [J]. Am J Sports Med, 2017, 45(4):826-831.
doi: 10.1177/0363546516674183 |
| [5] |
Clatworthy MG, Annear P, Bulow JU, et al. Tunnel widening in anterior cruciate ligament reconstruction: A prospective evaluation of hamstring and patella tendon grafts [J]. Knee Surg Sports Traumatol Arthrosc, 1999, 7(3):138-145.
doi: 10.1007/s001670050138 |
| [6] |
Fauno P, Kaalund S. Tunnel widening after hamstring anterior cruciate ligament reconstruction is influenced by the type of graft fixation used: A prospective randomized study [J]. Arthroscopy, 2005, 21(11):1337-1341.
doi: 10.1016/j.arthro.2005.08.023 |
| [7] |
Buelow JU, Siebold R, Ellermann A. A prospective evaluation of tunnel enlargement in anterior cruciate ligament reconstruction with hamstrings: Extracortical versus anatomical fixation [J]. Knee Surg Sports Traumatol Arthrosc, 2002, 10(2):80-85.
doi: 10.1007/s00167-001-0267-6 |
| [8] |
Wilson TC, Kantaras A, Atay A, et al. Tunnel enlargement after anterior cruciate ligament surgery [J]. Am J Sports Med, 2004, 32(2):543-549.
doi: 10.1177/0363546504263151 |
| [9] |
Fahey M, Indelicato PA. Bone tunnel enlargement after anterior cruciate ligament replacement [J]. Am J Sports Med, 1994, 22(3):410-414.
doi: 10.1177/036354659402200318 |
| [10] | Schulte K, Majewski M, Irrgang JJ, et al. Radiographic tunnel changes following arthroscopic ACL reconstruction: Autograft versus allograft [J]. Arthroscopy, 1996, 11(6):372-373. |
| [11] |
Hoher J, Moller HD, Fu FH. Bone tunnel enlargement after anterior cruciate ligament reconstruction: Fact or fiction? [J]. Knee Surg Sports Traumatol Arthrosc, 1998, 6(4):231-240.
doi: 10.1007/s001670050105 |
| [12] |
Buelow JU, Siebold R, Ellermann A. A new bicortical tibial fixation technique in anterior cruciate ligament reconstruction with quadruple hamstring graft [J]. Knee Surg Sports Traumatol Arthrosc, 2000, 8(4):218-225.
doi: 10.1007/s001670000120 |
| [13] |
Fink C, Zapp M, Benedetto KP, et al. Tibial tunnel enlargement following anterior cruciate ligament reconstruction with patellar tendon autograft [J]. Arthroscopy, 2001, 17(2):138-143.
pmid: 11172242 |
| [14] |
Webster KE, Feller JA, Hameister KA. Bone tunnel enlargement following anterior cruciate ligament reconstruction: A randomised comparison of hamstring and patellar tendon grafts with 2-year follow-up [J]. Knee Surg Sports Traumatol Arthrosc, 2001, 9(2):86-91.
doi: 10.1007/s001670100191 |
| [15] | Morgan CD, Stein DA, Leitman EH, et al. Anatomic tibial graft fixation using a retrograde bio-interference screw for endoscopic anterior cruciate ligament reconstruction [J]. Arthroscopy, 2002, 18(7):1-8. |
| [16] |
Jackson DW, Windler GE, Simon TM. Intraarticular reaction associated with the use of freeze-dried, ethylene oxide-sterilized bone-patella tendon-bone allografts in the reconstructuion of the anterior cruciate ligament [J]. Am J Sports Med, 1990, 18(1):1-11.
doi: 10.1177/036354659001800101 |
| [17] |
Zijl JA, Kleipool AE, Willems WJ. Comparison of tibial tunnel enlargement after anterior cruciate ligament reconstruction using patellar tendon autograft or allograft [J]. Am J Sports Med, 2000, 28(4):547-551.
doi: 10.1177/03635465000280041701 |
| [18] |
Cameron ML, Buchgraber A, Passler HH, et al. The natural hisroty of the anterior cruciate ligament-deficient knee. Changes in synovial fluid cytokine and keratan sulfate concentrations [J]. Am J Sports Med, 1997, 25(6):751-754.
doi: 10.1177/036354659702500605 |
| [19] |
Schamalzried TP, Akizuki KH, Fedenko AN, et al. The role of access of joint fluid to bone in periarticular osteolysis: A report of four cases [J]. J Bone Joint Surg, 1997, 79(3):447-452.
doi: 10.2106/00004623-199703000-00021 |
| [20] |
Beyaz S, Güler Üö, Demir S, et al. Tunnel widening after single versus doublebundle anterior cruciate ligament reconstruction: A randomized 8year followup study [J]. Arch Orthop Trauma Surg, 2017, 137(11):1547-1555.
doi: 10.1007/s00402-017-2774-z |
| [21] |
Flanigan DC, Everhart JS, DiBartola A, et al. Bacterial DNA is associated with tunnel widening in failed ACL reconstructions [J]. Knee Surg Sports Traumatol Arthrosc, 2019, 27(11):3490-3497.
doi: 10.1007/s00167-019-05405-6 |
| [22] |
Bjarnsholt T, Tolker-Nielsen T, Givskov M, et al. Detection of bacteria by fluorescence in situ hybridization in culture-negative soft tissue filler lesions [J]. Dermatol Surg, 2009, 35(2):1620-1624.
doi: 10.1111/j.1524-4725.2009.01313.x |
| [23] |
Everhart JS, DiBartola AC, Dusane DH, et al. Bacterial deoxyribonucleic acid is often present in failed revision anterior cruciate ligament reconstructions [J]. Arthroscopy, 2018, 34(11):3046-3052.
doi: S0749-8063(18)30521-8 pmid: 30301629 |
| [24] | Wise BT, Patel NN, Wier G, et al. Outcomes of ACL reconstruction with fixed versus variable loop button fixation [J]. Orthopedics, 2017, 40(2):e275-e280. |
| [25] |
Petre BM, Smith SD, Jansson KS, et al. Femoral cortical suspension devices for soft tissue anterior cruciate ligament reconstruction: A comparative biomechanical study [J]. Am J Sports Med, 2013, 41(2):416-422.
doi: 10.1177/0363546512469875 |
| [26] |
Barrow AE, Pilia M, Guda T, et al. Femoral suspension devices for anterior cruciate ligament reconstruction: Do adjustable loops lengthen? [J]. Am J Sports Med, 2014, 42(2):343-349.
doi: 10.1177/0363546513507769 pmid: 24158183 |
| [27] |
Johnson JS, Smith SD, LaPrade CM, et al. A biomechanical comparison of femoral cortical suspension devices for soft tissue anterior cruciate ligament reconstruction under high loads [J]. Am J Sports Med, 2015, 43(1):154-160.
doi: 10.1177/0363546514553779 pmid: 25326014 |
| [28] |
Ahn HW, SeonJK , Song EK, et al. Comparison of clinical and radiologic outcomes and second-look arthroscopic findings after anterior cruciate ligament reconstruction using fixed and adjustable loop cortical suspension devices [J]. Arthroscopy, 2019, 35(6):1736-1742.
doi: 10.1016/j.arthro.2019.01.051 |
| [29] | Iorio R, Di Sanzo V, Vadalà A, et al. ACL reconstruction with hamstrings: How different technique and fifixation devices influence bone tunnel enlargement [J]. Eur Rev Med Pharmacol Sci, 2013, 17(21):2956-2961. |
| [30] |
Lanzetti RM, Monaco E, de Carli A, et al. Can an adjustable-loop length suspensory fifixation device reduce femoral tunnel enlargement in anterior cruciate ligament reconstruction? A prospective computer tomography study [J]. Knee, 2016, 23(5):837-841.
doi: 10.1016/j.knee.2016.01.015 pmid: 27338510 |
| [1] | 任爽, 时会娟, 梁子轩, 张思, 胡晓青, 黄红拾, 敖英芳. 前交叉韧带重建术后侧切动作的生物力学特征[J]. 北京大学学报(医学版), 2024, 56(5): 868-873. |
| [2] | 王江静,魏顺依,敖英芳,杨渝平. 前交叉韧带重建术后三种不同药物镇痛早期疗效的对比[J]. 北京大学学报(医学版), 2024, 56(2): 293-298. |
| [3] | 任爽,时会娟,张家豪,刘振龙,邵嘉艺,朱敬先,胡晓青,黄红拾,敖英芳. 前交叉韧带重建术后移植物应力的有限元分析[J]. 北京大学学报(医学版), 2021, 53(5): 865-870. |
| [4] | 蒋艳芳,王健,王永健,刘佳,裴殷,刘晓鹏,敖英芳,马勇. 前交叉韧带翻修重建术后中长期临床疗效及影响因素[J]. 北京大学学报(医学版), 2021, 53(5): 857-863. |
| [5] | 张家豪,任爽,邵嘉艺,牛星跃,胡晓青,敖英芳. 前交叉韧带生物力学止点重建的解剖学与有限元分析[J]. 北京大学学报(医学版), 2019, 51(3): 586-590. |
|
||
