
1 资料与方法
1.1 一般资料

图1 各组肩袖撕裂患者的MRI影像Figure 1 MRI images of patients with rotator cuff tears in each group A, negative control group; B, partial RCTs (articular side) group; C, partial RCTs (bursal side) group; D, full-thickness RCTs group. The arrow indicates the site of RCTs, the circle marks the osteophytes of greater tuberosity of humerus. RCTs, rotator cuff tears. |
1.2 影像学测量及其他分析指标
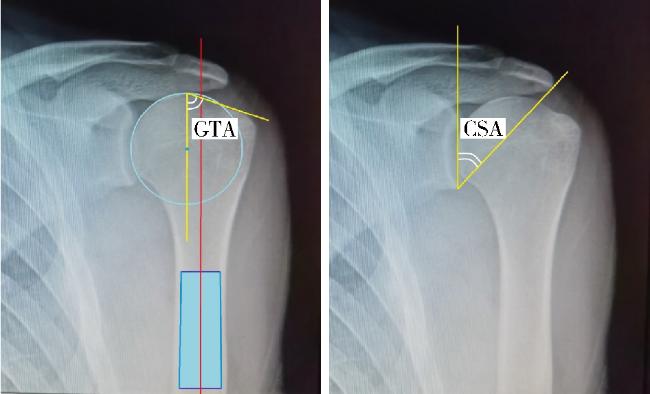
图2 GTA和CSA在肩胛骨正位X线片上的测量方法Figure 2 Measurement methods of GTA and CSA on apraxis of scapula Greater tuberosity angle (GTA) is made by two crossing lines. The first line passes through the center of humeral head and parallels to the humerus diaphysis, and the second one connects the upper border of the humeral head to the most superolateral edge of the greater tuberosity. Critical shoulder angle (CSA) consists of the angle with two crossing lines. One of which was drawn from the glenoid superior to inferior border, the other was drawn from the glenoid inferior border to lateral aspect of the acromion. |
1.3 统计学分析
2 结果
2.1 可靠性测试
表1 放射学测量的可靠性检测Table 1 Reliability of radiological measurements |
| Measurements | ICC-1 | ICC-2 | ICC-3 |
| CSA | 0.988 | 0.988 | 0.897 |
| GTA | 0.977 | 0.990 | 0.921 |
CSA, critical shoulder angle; GTA, greater tuberosity angle; ICC, intraclass correlation coefficient; ICC-1, surgeon intra-observer variation test; ICC-2, radiologist intra-observer variation test; ICC-3, surgeon vs. radiologist inter-observer variation test. |
2.2 RCTs患者特征的分析
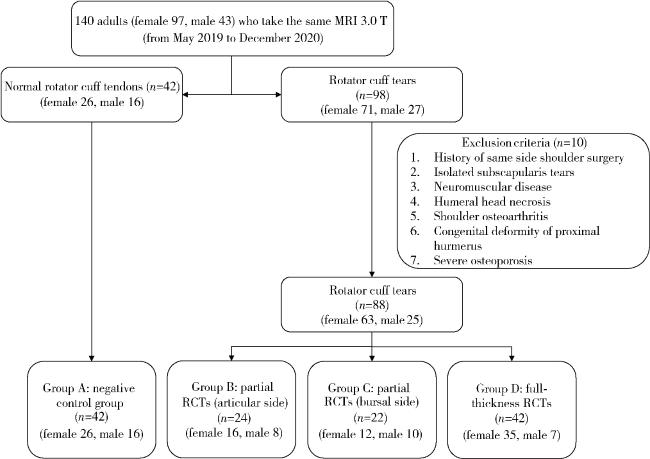
图3 受试者入组流程图Figure 3 Enrollment flow chart Patients were screened and grouped according to inclusion and exclusion criteria (according to the exclusion criteria, 10 patients with RCTs were not included in this study and statistical analysis due to factors such as preoperative imaging data missing (not recorded) and non-timely review. RCTs, rotator cuff tears. |
表2 各组人口学数据资料Table 2 Demographic data in each group |
| Items | Group A | Group B | Group C | Group D | P value |
| Age/years, ${\bar x}$±s | 27.76±7.30 | 54.00±14.89 | 51.27±8.41 | 64.24±10.01 | <0.001 |
| Weight/kg, ${\bar x}$±s | 58.90±6.51 | 63.83±9.06 | 63.27±6.13 | 61.43±10.06 | 0.075 |
| Height/m, ${\bar x}$±s | 1.64±0.50 | 1.65±0.78 | 1.62±0.68 | 1.59±0.07 | 0.001 |
| BMI/(kg/m2), ${\bar x}$±s | 21.82±1.73 | 23.24±1.91 | 24.04±1.54 | 24.10±2.93 | <0.001 |
| Gender (male/female), n | 16/26 | 8/16 | 10/12 | 7/35 | 0.067 |
| Shoulder (left/right), n | 16/26 | 8/16 | 12/10 | 18/24 | 0.487 |
| Smoking (yes/no), n | 6/36 | 2/22 | 2/20 | 2/40 | 0.511 |
Group A, negative control group; Group B, partial RCTs (articular side); Group C, partial RCTs (bursal side); Group D, full-thickness RCTs. RCTs, rotator cuff tears; BMI, body mass index. |
2.3 CSA和GTA的临界值分析
表3 各组CSA和GTA的测量值Table 3 Measured values of CSA and GTA in each group |
| Items | Group A | Group B | Group C | Group D |
| CSA, ${\bar x}$±s | 35.33±4.69 | 38.56±4.83 | 40.23±5.72 | 39.18±7.18 |
| GTA, ${\bar x}$±s | 68.36±3.06 | 70.54±3.08 | 71.09±5.31 | 72.62±5.37 |
The notes for Group A-D as in Table 2. GTA, greater tuberosity angle; CSA, critical shoulder angle. |
表4 CSA的组间多重比较(P value)Table 4 Multiple comparisons of CSA between groups (P value) |
| Items | Group A | Group B | Group C | Group D |
| Group A | - | 0.028* | 0.001** | 0.002** |
| Group B | 0.028* | - | 0.323 | 0.673 |
| Group C | 0.001** | 0.323 | - | 0.485 |
| Group D | 0.002** | 0.673 | 0.485 | - |
*, P<0.05; **, P<0.01. The notes for Group A-D as in Table 2. CSA, critical shoulder angle. |
表5 GTA的组间多重比较(P value)Table 5 Multiple comparisons of GTA between groups (P value) |
| Items | Group A | Group B | Group C | Group D |
| Group A | - | 0.045* | 0.015* | <0.001** |
| Group B | 0.045 | - | 0.660 | 0.057 |
| Group C | 0.015* | 0.660 | - | 0.172 |
| Group D | <0.001** | 0.057 | 0.172 | - |
*, P<0.05; **, P<0.01. The notes for Group A-D as in Table 2. GTA, greater tuberosity angle. |
2.4 CSA和GTA的相关性分析
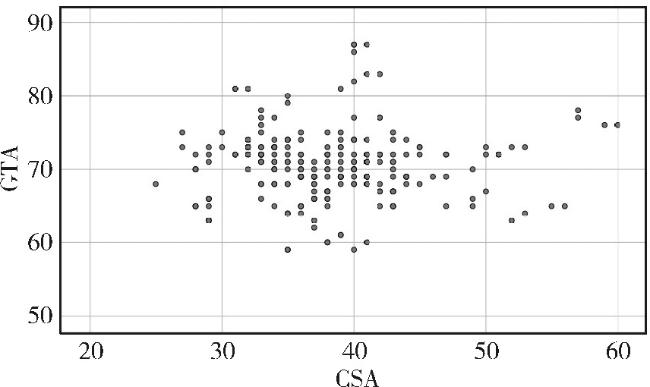
图5 GTA和CSA的散点图Figure 5 Scatter diagram of GTA and CSA GTA, greater tuberosity angle; CSA, critical shoulder angle. |
2.5 RCTs的危险因素和保护因素
表6 RCTs各组的优势比Table 6 Odd ratios of RCTs groups |
| Items | Group B | Group C | Group D | |||||
| OR (95%CI) | P value | OR (95%CI) | P value | OR (95%CI) | P value | |||
| Gender (male/female) | 1.231 (0.430-3.527) | 0.699 | 0.738 (0.260-2.100) | 0.569 | 3.077 (1.106-8.558) | 0.050 | ||
| Shoulder (left/right) | 1.231 (0.430-3.527) | 0.699 | 0.513 (0.180-1.458) | 0.208 | 0.821 (0.343-1.963) | 0.657 | ||
| Smoke (yes/no) | 1.833 (0.340-9.895) | 0.476 | 1.667 (0.307-9.042) | 0.551 | 3.333 (0.632-17.574) | 0.137 | ||
The notes for Group B-D as in Table 2. RCTs, rotator cuff tears. |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}