
近年来,全球罹患终末期肾病(end stage renal disease,ESRD)儿童(< 18岁)的发病率呈逐年上升趋势,美国肾脏数据系统(United States Renal Data System,USRDS)的报告显示,2021年美国0~17岁儿童ESRD的发病率为11.1/100万人[1]。根据我国医院质量监测系统(hospital quality monitoring system,HQMS)统计,2013年我国儿童慢性肾脏病(chronic kidney disease,CKD)住院人数为67 498人,2014年为76 810人,2015年为81 665人,2016年为82 649人,分别占儿童住院总数的1.93%、1.93%、1.99%和2.09%,其中,CKD进展为5期的平均发生率在35%以上,且呈逐年上升趋势[2]。
肾移植是ESRD患儿的最佳治疗方法[3],不仅可以显著改善ESRD患儿的生长发育,更重要的是能提高患儿的生活和生存质量[4]。北美儿科肾移植协作研究(North American Pediatric Renal Trials and Collaborative Study, NAPRTCS)的数据显示,接受肾脏替代治疗的患儿5年生存率为82%,而接受肾移植的患儿5年生存率为95%[5]。但是,由于儿童受者血管纤细、手术空间狭窄、术后管理复杂,导致儿童肾移植手术仍面临诸多挑战,特别是对于低龄(< 5岁)、低体重(< 15 kg)的患儿,肾移植仍是极具挑战的手术。本文报告北京大学人民医院2例低龄、低体重儿童的手术操作及临床管理经验,这2例手术均采用腹膜外途径手术方式,术后患儿肾功能恢复顺利,未出现手术相关并发症,并且在长期随访中取得良好结果。此外,本文还复习总结了来自多个国家和地区的低龄、低体重儿童肾移植手术的并发症发生率和长期随访结果,讨论此类特殊肾移植手术策略的选择,希望能为我国低龄、低体重儿童肾移植的发展提供借鉴。
1 病例资料
1.1 供受者一般资料
病例1,男,2岁3个月,在母孕24周的产前超声检查时提示双肾发育不良,行基因检测未发现致病基因。6个月前检查血肌酐500 μmol/L,双肾萎缩,即刻开始接受规律腹膜透析,但腹膜透析效率差。术前身高78 cm,体重8.8 kg,体重指数(body mass index,BMI)14.46 kg/m2。术前透析后血肌酐248 μmol/L,血尿素氮30.0 mmol/L,肾小球滤过率35.17 mL/(min·1.73 m2)。供肾者,男,6岁,身高130 cm,体重24 kg,BMI 14.2 kg/m2,腹部超声提示双肾无异常,左肾为供肾,人类白细胞抗原(human leukocyte antigen,HLA)错配数为3个,淋巴细胞毒交叉配合试验为1%。供者与受者年龄及BMI相仿。
病例2,女,3岁8个月,6个月前检查血肌酐600 μmol/L,生长发育迟缓,食欲不佳,肾性贫血,2个月前开始接受规律腹膜透析,术前身高85 cm,体重11.25 kg,BMI 15.57 kg/m2。术前透析后血肌酐281 μmol/L,血尿素氮16.0 mmol/L,肾小球滤过率22.63 mL/(min·1.73 m2)。供肾者,男,5岁,身高115 cm,体重20 kg,BMI 15.1 kg/m2,右肾为供肾,HLA错配数为3个,淋巴细胞毒交叉配合试验为2%。供者与受者年龄及BMI相仿。
1.2 移植前准备
免疫诱导:吗替麦考酚酯胶囊500 mg,巴利昔单抗10 mg(术前和术后第4天各给予10 mg),甲泼尼龙10 mg/kg。预防感染:美罗培南10 mg/kg;预防应激性溃疡:奥美拉唑1 mg/kg。
1.3 免疫维持方案
术后口服他克莫司0.15~0.20 mg/kg,每日两次;口服吗替麦考酚酯胶囊250 mg,每日两次。静脉输液甲泼尼龙:术后第1天10 mg/kg,术后第2天10 mg/kg,术后第3天5 mg/kg,术后第4天2.5 mg/kg,术后第5天改为口服20 mg。
1.4 围手术期情况
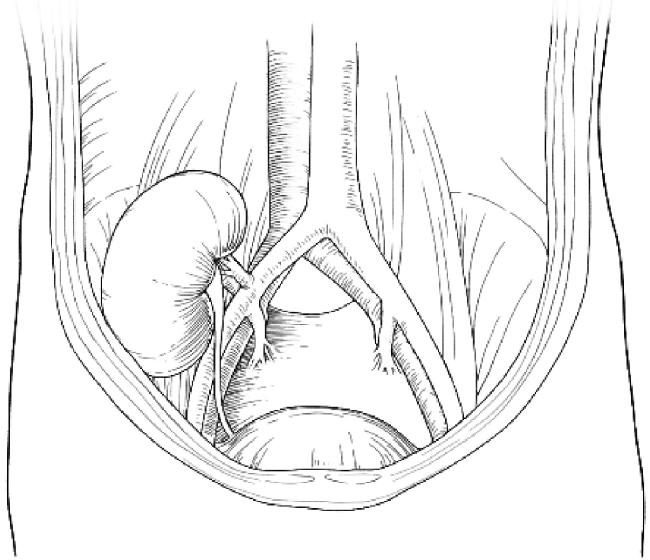
患儿(受者)麻醉成功后,取仰卧位,常规消毒、铺巾。取右下腹弧形切口,平脐水平,上段沿腹直肌外沿走行,下段向内,终于耻骨联合上缘,切口长约15 cm,逐层切开皮肤、皮下组织、腱膜及肌肉各层,进入腹膜外间隙。从右侧髂外动脉处将腹膜推向内上方,暴露右侧髂窝,显露髂总动脉、髂总静脉并仔细结扎所有覆盖于其表面的淋巴组织和结缔组织,将供肾放于右侧髂窝,供肾静脉和动脉分别与髂总静脉、髂总动脉行端侧吻合(图 1),供肾上极靠近腰大肌侧保留部分肾脏脂肪,用2-0可吸收线将肾周脂肪与腰大肌缝合固定,避免术后患儿哭闹导致肾脏扭转,易形成肾动脉血栓。血流开放后移植肾灌注良好,即刻输尿管断端有尿液排出,将移植肾输尿管与膀胱以隧道法吻合,留置D-J管1根[6]。最后在移植肾的上、下方各放置引流管1根,手术结束。
患儿术后移植肾的肾功能恢复顺利。病例1术后第3天血肌酐降至26 μmol/L,肾小球滤过率245.23 mL/(min·1.73 m2),术后13天痊愈出院,无排斥反应,术后无并发症发生。病例2术后第3天血肌酐降至39 μmol/L,肾小球滤过率164.12 mL/(min·1.73 m2),术后11天痊愈出院,无排斥反应,术后无并发症发生。
2 讨论
2.1 低龄、低体重儿童肾移植的发展现状
由于ESRD患儿生理和解剖结构上的特殊性以及手术技术的复杂性,儿童肾移植的普及率比成人更低。ESRD患儿在移植之前面临长期的透析治疗,但儿童透析水平的地区差异性更大,对医护人员的技术要求更高,同时,长期透析会给ESRD患儿带来营养不良等并发症,严重影响ESRD患儿的成长发育和心理健康。因此,推进发展儿童肾移植工作对改善ESRD患儿的生活质量具有重大意义。
儿童肾移植没有最小年龄的严格限制,ESRD患儿越早完成肾移植,越尽可能缩短肾脏替代的治疗时间,对患儿的长期存活越有利。已有研究发现,透析时间大于12个月的儿童出现移植物失功能的风险增高52%,透析时间大于18个月的儿童死亡风险增高89%[3],所以,在透析前尽早实施肾移植对患儿具有重要临床意义。但是,ESRD患儿年龄越小,面临的手术难度和临床管理的难度就越大,各种手术并发症的发生率也相对增加[7-8]。年龄 < 5岁,体重 < 15 kg的低龄、低体重ESRD患儿实施肾移植手术具有很大的临床挑战性。ESRD儿童常常伴有严重的营养不良和生长发育障碍问题,体重小于15 kg的患儿可能会有较大的年龄差异,因此体重比年龄能更好地反映其肾移植的管理难度[9],但同时,低龄儿童的依从性差,沟通与管理困难的特点也是医护人员必须面对的问题。随着外科技术的不断进步,世界范围内的医疗团队都在致力于挑战低龄、低体重患儿肾移植的极限。由于此类患儿血管较细、血管吻合难度高、供受者肾脏体积与腹腔比例差异大、患儿有效血管容量差异性大等多种因素均增加了手术难度,因此,合理选择恰当的手术策略,保证移植肾的有效灌注,对于减轻移植后并发症非常重要。
2.2 低龄、低体重儿童肾移植手术策略的选择
儿童肾移植主要有两种手术方法,一种为腹膜外途径,这种方式类似于成人肾移植,但也有一定区别,儿童肾移植的切口更偏上,主要是因为需要游离髂总动脉、髂总静脉,游离到更便于移植肾血管吻合的位置,而切口下缘离耻骨联合更远,主要原因是患儿膀胱的可塑性更好,膀胱充盈后位置可以更高,便于吻合;另一种手术方法为经腹腔内途径,采用腹部正中切口,于升结肠外侧沟剪开后腹膜,将升结肠和盲肠向中线推移,暴露腹主动脉下段与下腔静脉,将供肾动脉与腹主动脉行端侧吻合,供肾静脉与下腔静脉行端侧吻合,最后将移植肾放于腹腔内。
目前对于哪种手术方式最佳尚无定论,我国《儿童肾移植技术操作规范》推荐,体重小于10 kg的受者采用腹腔内途径,体重大于30 kg的受者采用腹膜外途径,处于两者之间的患者可根据实际情况选择手术方式[10]。在选择手术方式时主要需考虑以下因素:(1)充分考虑儿童生长发育的需要,尽量保留较大的动脉吻合口,避免日后生长过程中出现吻合口相对狭窄。(2)针对相对较大的移植肾,还需考虑供肾血流灌注的问题,如果吻合血管血流量不足,导致移植肾血供不足,将会出现与肾动脉狭窄类似的病理改变,因此,对于低龄、低体重的ESRD患儿,移植肾动脉吻合位置往往不能采用髂内外动脉,而是推荐将供肾动脉与受者髂总动脉行端侧吻合,若髂总动脉直径仍显著小于移植肾动脉直径,则推荐将供肾血管与腹主动脉进行端侧吻合,以保证移植肾有充足的血流[11]。对于儿童肾移植,我们常规采用髂内袖片技术,将供肾动脉与髂内动脉吻合,获得了很好的临床效果[12]。对于低龄、低体重ESRD患儿,我们采用供肾动静脉与髂总动静脉吻合方式,这种方式与髂内外血管吻合存在一定的手术差别:切口选择要超过平脐水平,下缘切口可以上移,切口长度并不需要特别扩大;髂总动脉常常可以充分游离,髂总静脉不需充分游离,使用侧壁钳部分阻断就可以;髂总动脉在内侧,髂总静脉在外侧,移植肾血管吻合时需要先完成动脉重建。(3)移植肾的放置方式也是必须考虑的重点。髂窝空间较腹腔内空间更小,如果供肾相对较大,更容易引起腹腔间隔室综合征,这是一种因多种因素导致腹腔内压力急性升高(腹内压≥20 mmHg),引起腹腔内外多器官系统功能受损的临床综合征,腹内压升高会导致肾血管阻力增加,中心静脉压、肺动脉压升高,腹内器官灌注不足,可以表现为腹胀、腹痛、恶心、呕吐、心悸、胸闷等[13-14],也会极大影响移植物的血供,引起血栓或移植物功能丧失[15]。但毕竟髂窝位置有助于移植肾位置的固定,可避免出现严重的血管弯折,增加血管并发症风险,而腹腔内放置更难固定移植肾。(4)如果在手术中对胃肠道刺激较多,会增加包括肠梗阻等在内的胃肠道并发症的发生率,这种情况在腹腔内手术更常见[16]。采用腹腔内途径手术时,由于需要阻断腹主动脉,相比阻断一侧髂血管,会增加酸中毒的程度[17]。(5)从术后长期的复查与随访角度来说,髂窝位置较为表浅,便于术后使用超声复查,如果出现手术并发症或严重排异反应,需要进行穿刺等临床操作时,也可以降低操作的难度,减少患儿受到的创伤。
2.3 相关文献回顾
随着移植技术的进步,儿童肾移植得到了长足的发展,但低龄、低体重患儿肾移植仍存在较多的风险。综合多个器官移植医学中心对低体重患儿肾移植的回顾性队列研究结果[8, 11, 18-30],手术相关并发症的中位发生率为14.0%(3.2%~26.0%),其中血管相关并发症(肾动脉血栓、肾静脉血栓、肾动脉狭窄等)的中位发生率为6.8%(0~22.2%),泌尿系统并发症(输尿管狭窄、尿瘘等)的中位发生率为5.3%(0~17.0%),供肾与患儿体重差异较大者可出现腹腔间隔室综合征,经腹腔内途径肾移植的患儿可出现肠梗阻等消化系统并发症。对进行长期随访的研究进行统计,移植物1年的中位存活率为93.5%(81.0%~98.4%),5年的中位存活率为87.0% (73.0%~96.6%),患者1年的中位生存率为98% (92%~100%),5年的中位生存率为96.0%(86.5%~ 99.1%)。
总之,随着儿童肾移植技术的不断发展,儿童肾移植的成功率和长期存活率也在不断提升。本研究对两例患者均进行了12个月的术后随访,由于处于免疫抑制状态,病例1出现了EB病毒(Epstein-Barr virus,EBV)和B19病毒感染,病例2出现了巨细胞病毒感染,但经过严密监测和及时干预,两例患者均未出现慢性移植肾功能不全。本研究通过总结2例低龄、低体重儿童肾移植的临床经验、手术经验,为低龄、低体重患儿这类特殊的肾移植手术提供了一些单中心经验,以期共同推动我国低体重儿童肾移植技术的发展。由于临床案例尚较少,对于低龄、低体重儿童肾移植的手术经验和技巧还需要更长时间的积累。

{kind=link}
{kind=link}