
1 资料与方法
1.1 研究对象
1.2 种植外科及修复方法
1.2.1 患者评估和术前设计
1.2.2 植入手术
1.3 临床随访和检查指标
1.3.1 种植体存留率
1.3.2 剩余牙槽骨及上颌窦解剖形态
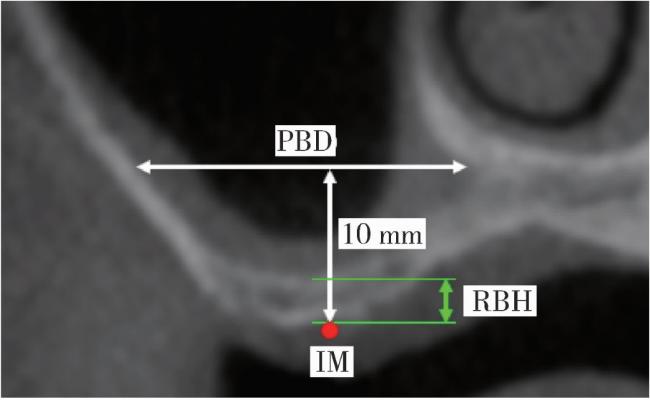
图2 RBH和PBD的测量Figure 2 Measurement of RBH and PBD IM, implantation point of zygomatic implant; PBD, distance between the palatal and buccal wall; RBH, residual bone height. |
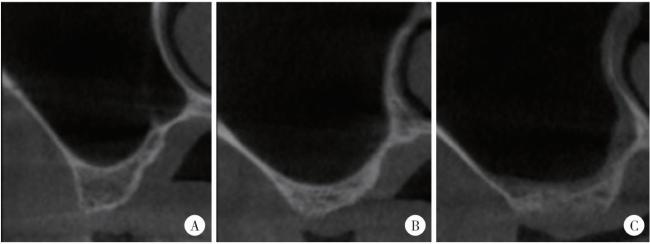
图3 上颌窦颊腭向轮廓Figure 3 Morphology of maxillary sinus in the buccal and palatal directions A, taper; B, round; C, flat. |
1.4 统计学方法
2 结果
2.1 患者及种植体一般资料
表1 患者一般资料(n=24)Table 1 General information of patients (n=24) |
| Items | Data |
| Gender, n(%) | |
| Male | 16 (66.7) |
| Female | 8 (33.3) |
| Age/years, n(%) | |
| 30- | 1 (4.2) |
| 40- | 8 (33.3) |
| 50- | 8 (33.3) |
| 60-69 | 7 (29.2) |
| General condition, n(%) | |
| Hypertension | 6 (25.0) |
| Diabetes | 2 (8.3) |
| Cardiovascular disease | 1 (4.2) |
| Smoking history, n(%) | 3 (12.5) |
表2 穿颧种植体一般资料(n=47)Table 2 General information of zygomatic implants (n=47) |
| Items | Data |
| Length of zygomatic implants/mm, ${\bar x}$±s | 43.78±4.91 |
| Site, n(%) | |
| Left | 24 (51.1) |
| Right | 23 (48.9) |
| Survival, n(%) | |
| No | 0 (0.0) |
| Yes | 47 (100.0) |
| Schneiderian membrane, n(%) | |
| Perforated | 10 (21.3) |
| Non-perforated | 37 (78.7) |
2.2 牙槽嵴及上颌窦解剖形态
2.2.1 RBH
表3 穿颧种植体的剩余牙槽骨高度Table 3 Residual bone height of zygomatic implants |
| Items | n | RBH/mm, median (IQR) | P |
| Gender | 0.025 | ||
| Male | 31 | 2.40 (1.70) | |
| Female | 16 | 3.90 (3.93) | |
| Site | 0.873 | ||
| Left | 24 | 2.60 (2.43) | |
| Right | 23 | 2.80 (2.20) | |
| Total | 47 | 2.80 (2.20) |
RBH, residual bone height; IQR, interquartile range. |
2.2.2 上颌窦颊腭向宽度和轮廓
2.3 上颌窦底成骨情况及影响因素
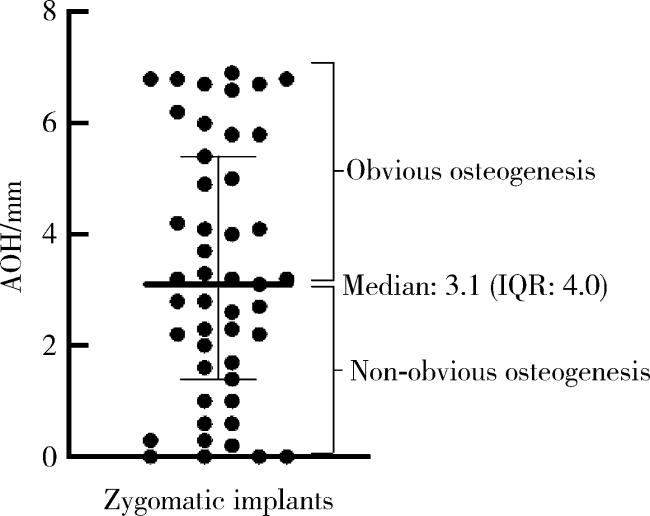
表4 上颌窦底成骨情况的单因素分析Table 4 Univariate analysis of osteogenesis of maxillary sinus floor |
| Examined variable | n | Obvious osteogenic rate/% | β | OR (95%CI) | P |
| Gender | |||||
| Male | 31 | 62.5 | Reference | ||
| Female | 16 | 41.9 | -0.842 | 0.43 (0.09, 1.52) | 0.197 |
| Age | 47 | 48.9 | 0.038 | 1.04 (0.96, 1.14) | 0.320 |
| Smoker | |||||
| No | 41 | 51.2 | Reference | ||
| Yes | 6 | 33.3 | -0.752 | 0.47 (0.05, 3.09) | 0.426 |
| Diabetes | |||||
| No | 43 | 48.8 | Reference | ||
| Yes | 4 | 50.0 | -0.002 | 1.00 (0.05, 9.37) | 0.998 |
| RBH | 47 | 48.9 | 0.738 | 2.09 (1.32, 4.57) | 0.006 |
| PBD | |||||
| Wide | 31 | 48.4 | Reference | ||
| Narrow | 16 | 50.0 | 0.094 | 1.10 (0.31, 5.44) | 0.886 |
| Morphology | |||||
| Round | 20 | 35.0 | Reference | ||
| Taper | 17 | 70.6 | 1.706 | 5.51 (0.84, 36.0) | 0.075 |
| Flat | 10 | 40.0 | 0.310 | 1.36 (0.23, 8.16) | 0.734 |
| Perforation | |||||
| No | 28 | 57.1 | Reference | ||
| Yes | 19 | 36.8 | -0.827 | 0.44 (0.13, 1.48) | 0.175 |
| Site | |||||
| Left | 24 | 50.0 | Reference | ||
| Right | 23 | 47.8 | -0.091 | 0.91 (0.28, 2.95) | 0.878 |
RBH, residual bone height; PBD, distance between the palatal and buccal wall. |
表5 上颌窦底成骨情况的多因素分析Table 5 Multivariate analysis of osteogenesis of maxillary sinus floor |
| Examined variables | β | OR (95%CI) | P | VIF |
| Morphology | ||||
| Round | Reference | |||
| Taper | 0.937 | 11.44 (1.11, 117.4) | 0.040 | 1.128 |
| RBH | 2.437 | 2.55 (1.14, 5.69) | 0.022 | 1.272 |
RBH, residual bone height; VIF, variance inflation factor. |
3 讨论
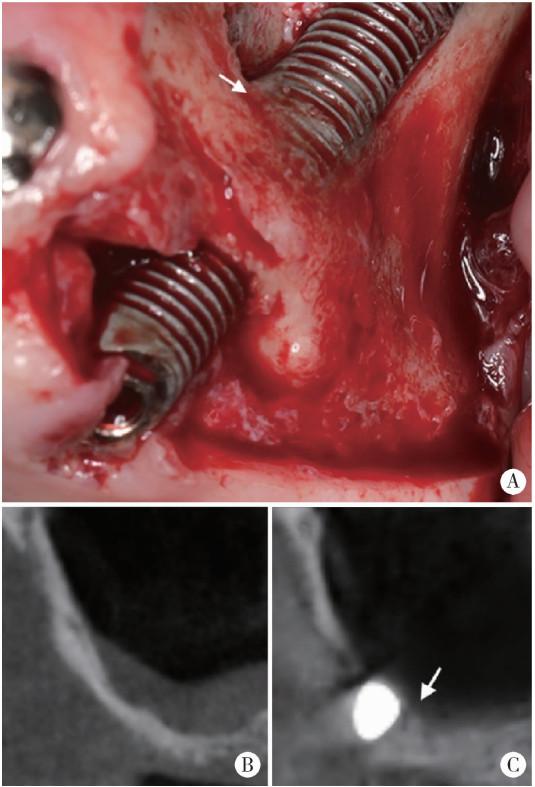
图6 1例颧周感染患者手术探查时发现上颌窦底成骨Figure 6 Osteogenesis of the maxillary sinus floor during surgical exploration in a patient with peri-zygomatic infection A, surgical exploration, arrow indicating new bone formation; B, pre-operative cone beam CT (CBCT); C, CBCT at 12 months after surgery, arrow indicating new bone formation. |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}