Journal of Peking University (Health Sciences) ›› 2022, Vol. 54 ›› Issue (1): 62-67. doi: 10.19723/j.issn.1671-167X.2022.01.010
Previous Articles Next Articles
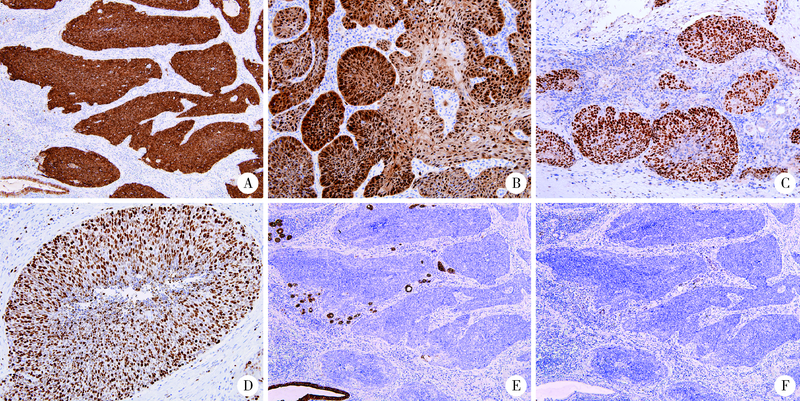
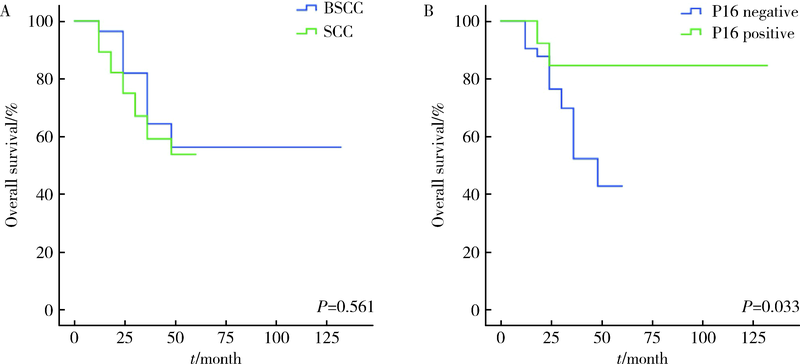
Clinicopathological study in 28 cases of oral basaloid squamous cell carcinomas
ZHOU Chuan-xiang,ZHOU Zheng,ZHANG Ye,LIU Xiao-xiao,GAO Yan( )
)
- Department of Oral Pathology, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
CLC Number:
- R780.2



| [1] |
Wain SL, Kier R, Vollmer RT, et al. Basaloid-squamous carcinoma of the tongue, hypopharynx, and larynx: report of 10 cases[J]. Hum Pathol, 1986, 17(11):1158-1166.
pmid: 3770734 |
| [2] |
Paulino AF, Singh B, Shah JP, et al. Basaloid squamous cell carcinoma of the head and neck[J]. Laryngoscope, 2000, 110(9):1479-1482.
pmid: 10983946 |
| [3] |
Soriano E, Faure C, Lantuejoul S, et al. Course and prognosis of basaloid squamous cell carcinoma of the head and neck: a case-control study of 62 patients[J]. Eur J Cancer, 2008, 44(2):244-250.
doi: 10.1016/j.ejca.2007.11.008 |
| [4] |
Ramqvist T, Näsman A, Franzeén B, et al. Protein expression in tonsillar and base of tongue cancer and in relation to human papillomavirus (HPV) and clinical outcome.[J]. Int J Mol Sci, 2018, 19(4):978.
doi: 10.3390/ijms19040978 |
| [5] | Näsman A, Bersani C, Lindquist D, et al. Human papillomavirus and potentially relevant biomarkers in tonsillar and base of tongue squamous cell carcinoma[J]. Anticancer Res, 2017, 37(10):5319-5328. |
| [6] |
Xu Y, Zhao H, Tong Y, et al. Comparative analysis of clinicopathological characteristics, survival features, and protein expression between basaloid and squamous cell carcinoma of the esophagus[J]. Int J Gen Med, 2021, 14:3929-3939.
doi: 10.2147/IJGM.S314054 |
| [7] |
Linton OR, Moore MG, Brigance JS, et al. Prognostic significance of basaloid squamous cell carcinoma in head and neck can-cer[J]. JAMA Otolaryngol Head Neck Surg, 2013, 139(12):1306-1311.
doi: 10.1001/jamaoto.2013.5308 |
| [8] |
Thariat J, Badoual C, Faure C, et al. Basaloid squamous cell carcinoma of the head and neck: role of HPV and implication in treatment and prognosis[J]. J Clin Pathol, 2010, 63(10):857-866.
doi: 10.1136/jcp.2010.078154 pmid: 20876315 |
| [9] |
de Sampaio Góes FC, Oliveira DT, Dorta RG, et al. Prognoses of oral basaloid squamous cell carcinomas and squamous cell carcinoma: a comparison[J]. Arch Otolaryngol Head Neck Surg, 2004, 130(1):83-86.
doi: 10.1001/archotol.130.1.83 |
| [10] |
Yu GY, Gao Y, Peng X, et al. A clinicopathologic study on basaloid squamous cell carcinoma in the oral and maxillofacial region[J]. Int J Oral Maxillofac Surg, 2008, 37(11):1003-1008.
doi: 10.1016/j.ijom.2008.05.019 |
| [11] | 代璐岭, 杨秀秀, 赵好为, 等. 牙龈基底细胞样鳞状细胞癌1例[J]. 华西口腔医学杂志, 2020, 38(3):347-350. |
| [12] | Sato F, Bhawal UK, Tojyo I, et al. Differential expression of claudin-4, occludin, SOX2 and proliferating cell nuclear antigen between basaloid squamous cell carcinoma and squamous cell carcinoma[J]. Mol Med Rep, 2019, 20(2):1977-1985. |
| [13] |
Schuch LF, Nóbrega KHS, Gomes APN, et al. Basaloid squamous cell carcinoma: a 31-year retrospective study and analysis of 214 cases reported in the literature[J]. Oral Maxillofac Surg, 2020, 24(1):103-108.
doi: 10.1007/s10006-020-00828-9 |
| [14] |
Lee JH, Kang HJ, Yoo CW, et al. PLAG1, SOX10, and Myb expression in benign and malignant salivary gland neoplasms[J]. J Pathol Transl Med, 2019, 53(1):23-30.
doi: 10.4132/jptm.2018.10.12 |
| [15] |
Hsieh MS, Lee YH, Chang YL. SOX10-positive salivary gland tumors: a growing list, including mammary analogue secretory carcinoma of the salivary gland, sialoblastoma, low-grade salivary duct carcinoma, basal cell adenoma/adenocarcinoma, and a subgroup of mucoepidermoid carcinoma[J]. Hum Pathol, 2016, 56:134-142.
doi: 10.1016/j.humpath.2016.05.021 |
| [16] |
Adkins BD, Geromes A, Zhang LY, et al. SOX10 and GATA3 in adenoid cystic carcinoma and polymorphous adenocarcinoma[J]. Head Neck Pathol, 2020, 14(2):406-411.
doi: 10.1007/s12105-019-01046-w pmid: 31222589 |
| [17] |
Nakaguro M, Tada Y, Faquin WC, et al. Salivary duct carcinoma: updates in histology, cytology, molecular biology, and treatment[J]. Cancer Cytopathol, 2020, 128(10):693-703.
doi: 10.1002/cncy.22288 pmid: 32421944 |
| [18] |
Boon E, Bel M, van Boxtel W, et al. A clinicopathological study and prognostic factor analysis of 177 salivary duct carcinoma patients from The Netherlands[J]. Int J Cancer, 2018, 143(4):758-766.
doi: 10.1002/ijc.31353 |
| [19] |
Santana T, Pavel A, Martinek P, et al. Biomarker immunoprofile and molecular characteristics in salivary duct carcinoma: clinicopathological and prognostic implications[J]. Hum Pathol, 2019, 93:37-47.
doi: 10.1016/j.humpath.2019.08.009 |
| [20] |
Villada G, Kryvenko ON, Campuzano-Zuluaga G, et al. A limited immunohistochemical panel to distinguish basal cell carcinoma of cutaneous origin from basaloid squamous cell carcinoma of the head and neck[J]. Appl Immunohistochem Mol Morphol, 2018, 26(2):126-131.
doi: 10.1097/PAI.0000000000000394 |
| [21] |
Mendelsohn AH, Lai CK, Shintaku IP, et al. Histopathologic findings of HPV and p16 positive HNSCC[J]. Laryngoscope, 2010, 120(9):1788-1794.
doi: 10.1002/lary.21044 |
| [22] |
Begum S, Westra WH. Basaloid squamous cell carcinoma of the head and neck is a mixed variant that can be further resolved by HPV status[J]. Am J Surg Pathol, 2008, 32(7):1044-1050.
doi: 10.1097/PAS.0b013e31816380ec |
| [23] |
Lai K, Killingsworth M, Matthews S, et al. Differences in survival outcome between oropharyngeal and oral cavity squamous cell carcinoma in relation to HPV status[J]. J Oral Pathol Med, 2017, 46(8):574-582.
doi: 10.1111/jop.2017.46.issue-8 |
| [24] |
Duncan LD, Winkler M, Carlson ER, et al. P16 immunohistochemistry can be used to detect human papillomavirus in oral cavity squamous cell carcinoma[J]. J Oral Maxillofac Surg, 2013, 71(8):1367-1375.
doi: 10.1016/j.joms.2013.02.019 |
| [1] | Junqi SU,Xiaoying WANG,Zhiqiang SUN. Establishment and verification of a prognostic nomogram for survival of tongue squamous cell carcinoma patients who underwent cervical dissection [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 120-130. |
| [2] | Han LU,Jian-yun ZHANG,Rong YANG,Le XU,Qing-xiang LI,Yu-xing GUO,Chuan-bin GUO. Clinical factors affecting the prognosis of lower gingival squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 702-707. |
| [3] | SU Jun-qi,SONG Yang,XIE Shang. Analysis of etiological characteristics and establishment of prediction model of postoperative infections in patients undergoing oral squamous cell carcinoma surgery with free flap reconstruction [J]. Journal of Peking University (Health Sciences), 2022, 54(1): 68-76. |
| [4] | Lei-zhen SU,Jie CHEN,Xian LI,Ping JI. Effects of salinomycin on proliferation and apoptosis of oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2020, 52(5): 902-906. |
| [5] | Chuan-si-bo TAO,Fan DONG,Dian-can WANG,Chuan-bin GUO. Diagnostic test for detection of cervical lymph node metastasis from oral squamous cell carcinoma via infrared thermal imaging [J]. Journal of Peking University(Health Sciences), 2019, 51(5): 959-963. |
| [6] | Yang LIU,Yan GAO,Xue-jie CHEN,Hong HUA. DNA cytometry of exfoliated cells in the diagnosis of oral potential malignant disorders [J]. Journal of Peking University(Health Sciences), 2019, 51(1): 16-20. |
| [7] | Chun-feng ZHANG,Yun LIU,Min LU,Xiao-juan DU. Expression of hUTP14a in non-small cell lung cancer [J]. Journal of Peking University(Health Sciences), 2019, 51(1): 145-150. |
|
||