Journal of Peking University (Health Sciences) ›› 2022, Vol. 54 ›› Issue (1): 54-61. doi: 10.19723/j.issn.1671-167X.2022.01.009
Previous Articles Next Articles
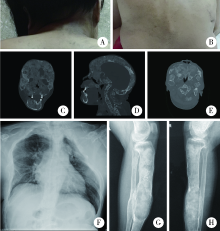
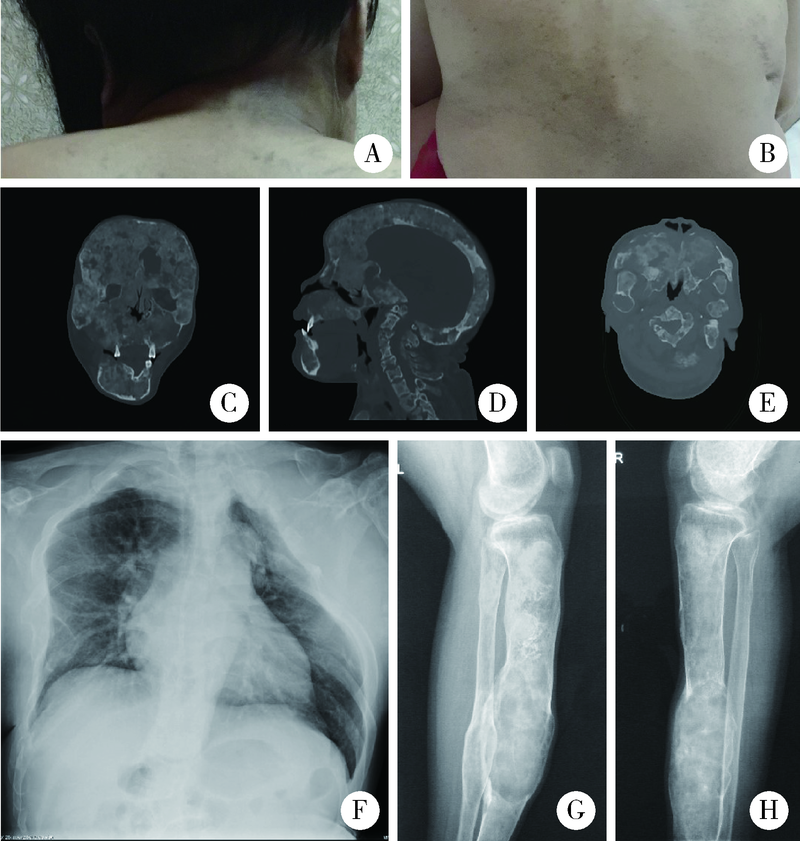
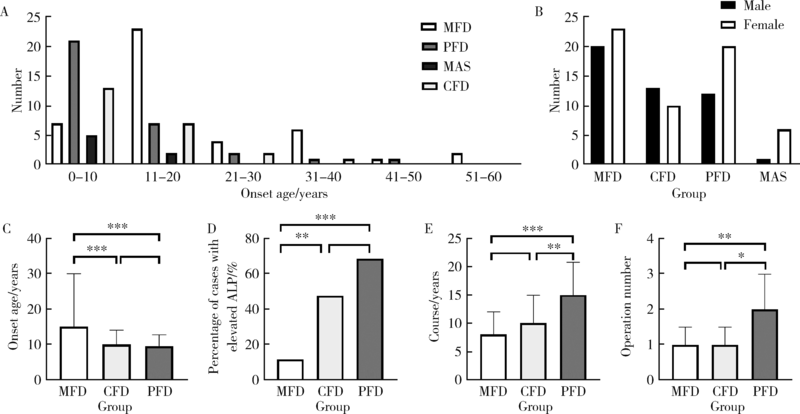
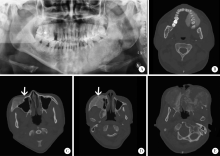
Clinicopathological analysis of 105 patients with fibrous dysplasia of cranio-maxillofacial region
XUE Jiang1,ZHANG Jian-yun1,SHI Rui-rui2,XIE Xiao-yan3,BAI Jia-ying1,LI Tie-jun1,△( )
)
- 1. Department of Oral Pathology, Peking University School and Hospital of Stomatology, Beijing 100081, China
2. Central Laboratory, Peking University School and Hospital of Stomatology, Beijing 100081, China
3. Department of Oral and Maxillofacial Radiology, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
CLC Number:
- R739.8

| [1] |
Dumitrescu CE, Collins MT. McCune-Albright syndrome[J]. Orphanet J Rare Dis, 2008, 3:12.
doi: 10.1186/1750-1172-3-12 pmid: 18489744 |
| [2] | 叶为民, 竺涵光, 郑家伟, 等. 46例颌面部骨纤维异常增殖症临床分析[J]. 中国口腔颌面外科杂志, 2008, 6(3):170-173. |
| [3] | El-Naggar AK, Chan JK, Grandis JR, et al. WHO classification of head and neck tumours [M]. Lyon: IARC Press, 2017: 253-254. |
| [4] | 张壁, 韩其滨, 赵吉宏, 等. 30例颌面部骨纤维异常增殖症诊治的临床分析[J]. 口腔医学研究, 2010, 26(5):713-715. |
| [5] |
Sweeney K, Kaban LB. Natural history and progression of craniofacial fibrous dysplasia: A retrospective evaluation of 114 patients from Massachusetts General Hospital[J]. J Oral Maxillofac Surg, 2020, 78(11):1966-1980.
doi: 10.1016/j.joms.2020.05.036 |
| [6] |
Cheng J, Wang Y, Yu H, et al. An epidemiological and clinical analysis of craniomaxillofacial fibrous dysplasia in a Chinese population[J]. Orphanet J Rare Dis, 2012, 7:80.
doi: 10.1186/1750-1172-7-80 pmid: 23074969 |
| [7] |
Javaid MK, Boyce A, Appelman-Dijkstra N, et al. Best practice management guidelines for fibrous dysplasia/McCune-Albright syndrome: A consensus statement from the FD/MAS international consortium[J]. Orphanet J Rare Dis, 2019, 14(1):139.
doi: 10.1186/s13023-019-1102-9 |
| [8] | World Health Organization. WHO classification of tumours of soft tissue and bone [M]. 5th ed. Lyon: IARC Press, 2020: 472-474. |
| [9] |
Ma J, Liang L, Gu B, et al. A retrospective study on craniofacial fibrous dysplasia: Preoperative serum alkaline phosphatase as a prognostic marker?[J]. J Craniomaxillofac Surg, 2013, 41(7):644-647.
doi: 10.1016/j.jcms.2012.12.007 |
| [10] | Chen YR, Wong FH, Hsueh C, et al. Computed tomography characteristics of non-syndromic craniofacial fibrous dysplasia[J]. Chang Gung Med J, 2002, 25(1):1-8. |
| [11] |
Burke AB, Collins MT, Boyce AM. Fibrous dysplasia of bone: Craniofacial and dental implications[J]. Oral Dis, 2017, 23(6):697-708.
doi: 10.1111/odi.12563 pmid: 27493082 |
| [12] |
Akintoye SO, Lee JS, Feimster T, et al. Dental characteristics of fibrous dysplasia and McCune-Albright syndrome[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2003, 96(3):275-282.
doi: 10.1016/S1079-2104(03)00225-7 |
| [13] |
Waldron CA. Fibro-osseous lesions of the jaws[J]. J Oral Maxillofac Surg, 1993, 51(8):828-835.
doi: 10.1016/S0278-2391(10)80097-7 |
| [14] |
Gupta D, Garg P, Mittal A. Computed tomography in craniofacial fibrous dysplasia: A case series with review of literature and classification update[J]. Open Dent J, 2017, 11:384-403.
doi: 10.2174/1874210601711010384 |
| [15] | 李铁军. 口腔组织学与病理学 [M]. 3版. 北京: 北京大学医学出版社, 2020: 360-361. |
| [16] |
Slootweg PJ. Maxillofacial fibro-osseous lesions: Classification and differential diagnosis[J]. Semin Diagn Pathol, 1996, 13(2):104-112.
pmid: 8734416 |
| [17] |
Riminucci M, Liu B, Corsi A, et al. The histopathology of fibrous dysplasia of bone in patients with activating mutations of the Gs alpha gene: Site-specific patterns and recurrent histological hallmarks[J]. J Pathol, 1999, 187(2):249-258.
pmid: 10365102 |
| [18] |
Sissons HA, Steiner GC, Dorfman HD. Calcified spherules in fibro-osseous lesions of bone[J]. Arch Pathol Lab Med, 1993, 117(3):284-290.
pmid: 8442673 |
| [19] | Dorfman HD. New knowledge of fibro-osseous lesions of bone[J]. Int J Surg Pathol, 2010, 18(3 Suppl):62S-65S. |
| [20] |
Sargolzaei S, Ghelejkhani A, Baghban AA. Diagnostic and bio-logical significance of immunohistochemical expression of osteopontin and Ki67 in fibro-osseous lesions of jaws[J]. J Islam Dent Assoc IRAN, 2017, 29(2):70-78.
doi: 10.30699/jidai.29.2.70 |
| [21] |
Shi RR, Li XF, Zhang R, et al. GNAS mutational analysis in differentiating fibrous dysplasia and ossifying fibroma of the jaw[J]. Mod Pathol, 2013, 26(8):1023-1031.
doi: 10.1038/modpathol.2013.31 |
| [22] |
Li Z, Raynald, Wang Z, et al. Malignant transformation of craniofacial fibrous dysplasia: A systematic review of overall survival[J]. Neurosurg Rev, 2020, 43(3):911-921.
doi: 10.1007/s10143-019-01089-1 |
| [1] | Han ZHANG, Fujia YANG, Ruili YANG. Progress in regulating stem cell functions for repair and regeneration of craniomaxillofacial tissues [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 285-289. |
| [2] | Xiaolin WANG, Luyao LI, Wen ZHANG, Hongyan WANG. Clinicopathological analysis of mesonephric-like adenocarcinoma in the corpusuteri: A report of 3 cases [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1208-1212. |
| [3] | Jianjun SUN, Qianquan MA, Xiaoliang YIN, Chenlong YANG, Jia ZHANG, Suhua CHEN, Chao WU, Jingcheng XIE, Yunfeng HAN, Guozhong LIN, Yu SI, Jun YANG, Haibo WU, Qiang ZHAO. Significance of precise classification of sacral meningeal cysts by multiple dimensions radiographic reconstruction MRI in guiding operative strategy and rehabilitation [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 303-308. |
| [4] | Guangyan YU, Xin PENG, Min GAO, Peng YE, Na GE, Mengqi JIA, Bingyu LI, Zunan TANG, Leihao HU, Wenbo ZHANG. Research progress in diagnosis and treatment of salivary gland tumors [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 1-6. |
| [5] | Hongyan WANG, Xinming LI, Kechi FANG, Huaqun ZHU, Rulin JIA, Jing WANG. Analysis of characteristics related to the disease activity of systemic lupus erythematosus and construction of an evaluation model [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1017-1022. |
| [6] | Jialu CHE, Zichen LIU, Kun LI, Chen ZHANG, Nanying CHE. Clinical value of automated EasyNAT system for the diagnosis of tuberculosis in paraffin-embedded tissues [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1047-1051. |
| [7] | Liang ZHAO, Chenglong SHI, Ke MA, Jing ZHAO, Xiao WANG, Xiaoyan XING, Wanxing MO, Yirui LIAN, Chao GAO, Yuhui LI. Immunological characteristics of patients with anti-synthetase syndrome overlap with rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 972-979. |
| [8] | Dongwu LIU, Jie CHEN, Mingli GAO, Jing YU. Rheumatoid arthritis with Castleman-like histopathology in lymph nodes: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 928-931. |
| [9] | Yuxuan TIAN,Mingjian RUAN,Yi LIU,Derun LI,Jingyun WU,Qi SHEN,Yu FAN,Jie JIN. Predictive effect of the dual-parametric MRI modified maximum diameter of the lesions with PI-RADS 4 and 5 on the clinically significant prostate cancer [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 567-574. |
| [10] | Zhanhong LAI,Jiachen LI,Zelin YUN,Yonggang ZHANG,Hao ZHANG,Xiaoyan XING,Miao SHAO,Yuebo JIN,Naidi WANG,Yimin LI,Yuhui LI,Zhanguo LI. A unicenter real-world study of the correlation factors for complete clinical response in idiopathic inflammatory myopathies [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 284-292. |
| [11] | Xunmin XU,Xiao SHAO,Aiping JI. Analysis of death cases in the oral emergency department [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 185-189. |
| [12] | Lu FENG,Jia-yu ZHAI,Jin-xia ZHAO. Medical visit status and clinical features in patients with IgG4 related disease [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1028-1032. |
| [13] | Hui WEI, Ci-dan-yang-zong, Yi-xi-la-mu, Bai-ma-yang-jin. Risk factors associated with different types of Henoch-Schönlein purpura in Tibetan patients at high altitude [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 923-928. |
| [14] | Yun-fei SHI,Hao-jie WANG,Wei-ping LIU,Lan MI,Meng-ping LONG,Yan-fei LIU,Yu-mei LAI,Li-xin ZHOU,Xin-ting DIAO,Xiang-hong LI. Analysis of clinicopathological and molecular abnormalities of angioimmunoblastic T-cell lymphoma [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 521-529. |
| [15] | Li-jia MA,Pan-pan HU,Xiao-guang LIU. Spinal metastases combined with leptomeningeal metastasis: A case report [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 563-566. |
|
||