Journal of Peking University (Health Sciences) ›› 2022, Vol. 54 ›› Issue (1): 62-67. doi: 10.19723/j.issn.1671-167X.2022.01.010
Previous Articles Next Articles
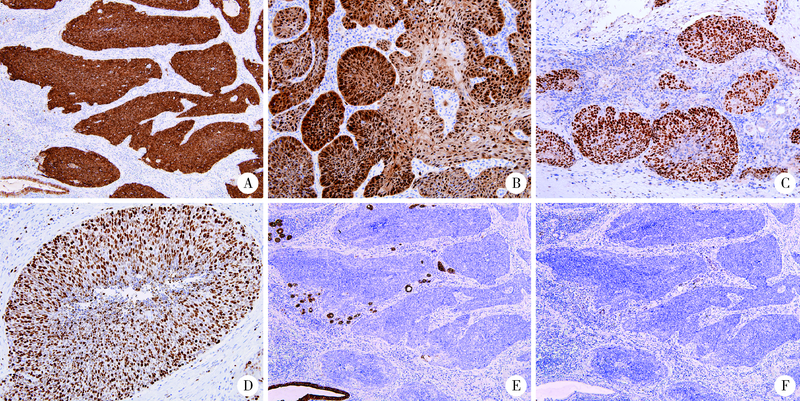
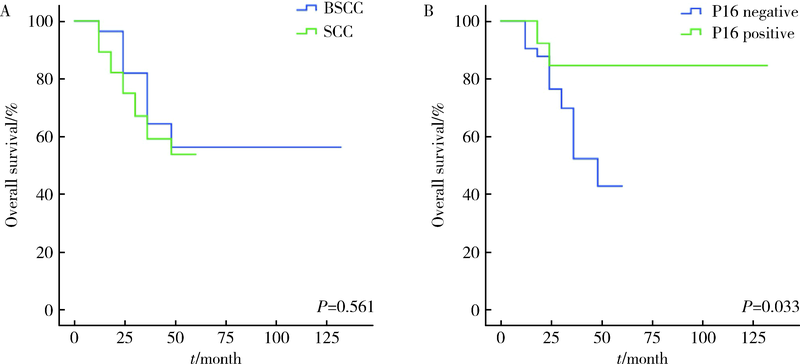
Clinicopathological study in 28 cases of oral basaloid squamous cell carcinomas
ZHOU Chuan-xiang,ZHOU Zheng,ZHANG Ye,LIU Xiao-xiao,GAO Yan( )
)
- Department of Oral Pathology, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
CLC Number:
- R780.2



| [1] |
Wain SL, Kier R, Vollmer RT, et al. Basaloid-squamous carcinoma of the tongue, hypopharynx, and larynx: report of 10 cases[J]. Hum Pathol, 1986, 17(11):1158-1166.
pmid: 3770734 |
| [2] |
Paulino AF, Singh B, Shah JP, et al. Basaloid squamous cell carcinoma of the head and neck[J]. Laryngoscope, 2000, 110(9):1479-1482.
pmid: 10983946 |
| [3] |
Soriano E, Faure C, Lantuejoul S, et al. Course and prognosis of basaloid squamous cell carcinoma of the head and neck: a case-control study of 62 patients[J]. Eur J Cancer, 2008, 44(2):244-250.
doi: 10.1016/j.ejca.2007.11.008 |
| [4] |
Ramqvist T, Näsman A, Franzeén B, et al. Protein expression in tonsillar and base of tongue cancer and in relation to human papillomavirus (HPV) and clinical outcome.[J]. Int J Mol Sci, 2018, 19(4):978.
doi: 10.3390/ijms19040978 |
| [5] | Näsman A, Bersani C, Lindquist D, et al. Human papillomavirus and potentially relevant biomarkers in tonsillar and base of tongue squamous cell carcinoma[J]. Anticancer Res, 2017, 37(10):5319-5328. |
| [6] |
Xu Y, Zhao H, Tong Y, et al. Comparative analysis of clinicopathological characteristics, survival features, and protein expression between basaloid and squamous cell carcinoma of the esophagus[J]. Int J Gen Med, 2021, 14:3929-3939.
doi: 10.2147/IJGM.S314054 |
| [7] |
Linton OR, Moore MG, Brigance JS, et al. Prognostic significance of basaloid squamous cell carcinoma in head and neck can-cer[J]. JAMA Otolaryngol Head Neck Surg, 2013, 139(12):1306-1311.
doi: 10.1001/jamaoto.2013.5308 |
| [8] |
Thariat J, Badoual C, Faure C, et al. Basaloid squamous cell carcinoma of the head and neck: role of HPV and implication in treatment and prognosis[J]. J Clin Pathol, 2010, 63(10):857-866.
doi: 10.1136/jcp.2010.078154 pmid: 20876315 |
| [9] |
de Sampaio Góes FC, Oliveira DT, Dorta RG, et al. Prognoses of oral basaloid squamous cell carcinomas and squamous cell carcinoma: a comparison[J]. Arch Otolaryngol Head Neck Surg, 2004, 130(1):83-86.
doi: 10.1001/archotol.130.1.83 |
| [10] |
Yu GY, Gao Y, Peng X, et al. A clinicopathologic study on basaloid squamous cell carcinoma in the oral and maxillofacial region[J]. Int J Oral Maxillofac Surg, 2008, 37(11):1003-1008.
doi: 10.1016/j.ijom.2008.05.019 |
| [11] | 代璐岭, 杨秀秀, 赵好为, 等. 牙龈基底细胞样鳞状细胞癌1例[J]. 华西口腔医学杂志, 2020, 38(3):347-350. |
| [12] | Sato F, Bhawal UK, Tojyo I, et al. Differential expression of claudin-4, occludin, SOX2 and proliferating cell nuclear antigen between basaloid squamous cell carcinoma and squamous cell carcinoma[J]. Mol Med Rep, 2019, 20(2):1977-1985. |
| [13] |
Schuch LF, Nóbrega KHS, Gomes APN, et al. Basaloid squamous cell carcinoma: a 31-year retrospective study and analysis of 214 cases reported in the literature[J]. Oral Maxillofac Surg, 2020, 24(1):103-108.
doi: 10.1007/s10006-020-00828-9 |
| [14] |
Lee JH, Kang HJ, Yoo CW, et al. PLAG1, SOX10, and Myb expression in benign and malignant salivary gland neoplasms[J]. J Pathol Transl Med, 2019, 53(1):23-30.
doi: 10.4132/jptm.2018.10.12 |
| [15] |
Hsieh MS, Lee YH, Chang YL. SOX10-positive salivary gland tumors: a growing list, including mammary analogue secretory carcinoma of the salivary gland, sialoblastoma, low-grade salivary duct carcinoma, basal cell adenoma/adenocarcinoma, and a subgroup of mucoepidermoid carcinoma[J]. Hum Pathol, 2016, 56:134-142.
doi: 10.1016/j.humpath.2016.05.021 |
| [16] |
Adkins BD, Geromes A, Zhang LY, et al. SOX10 and GATA3 in adenoid cystic carcinoma and polymorphous adenocarcinoma[J]. Head Neck Pathol, 2020, 14(2):406-411.
doi: 10.1007/s12105-019-01046-w pmid: 31222589 |
| [17] |
Nakaguro M, Tada Y, Faquin WC, et al. Salivary duct carcinoma: updates in histology, cytology, molecular biology, and treatment[J]. Cancer Cytopathol, 2020, 128(10):693-703.
doi: 10.1002/cncy.22288 pmid: 32421944 |
| [18] |
Boon E, Bel M, van Boxtel W, et al. A clinicopathological study and prognostic factor analysis of 177 salivary duct carcinoma patients from The Netherlands[J]. Int J Cancer, 2018, 143(4):758-766.
doi: 10.1002/ijc.31353 |
| [19] |
Santana T, Pavel A, Martinek P, et al. Biomarker immunoprofile and molecular characteristics in salivary duct carcinoma: clinicopathological and prognostic implications[J]. Hum Pathol, 2019, 93:37-47.
doi: 10.1016/j.humpath.2019.08.009 |
| [20] |
Villada G, Kryvenko ON, Campuzano-Zuluaga G, et al. A limited immunohistochemical panel to distinguish basal cell carcinoma of cutaneous origin from basaloid squamous cell carcinoma of the head and neck[J]. Appl Immunohistochem Mol Morphol, 2018, 26(2):126-131.
doi: 10.1097/PAI.0000000000000394 |
| [21] |
Mendelsohn AH, Lai CK, Shintaku IP, et al. Histopathologic findings of HPV and p16 positive HNSCC[J]. Laryngoscope, 2010, 120(9):1788-1794.
doi: 10.1002/lary.21044 |
| [22] |
Begum S, Westra WH. Basaloid squamous cell carcinoma of the head and neck is a mixed variant that can be further resolved by HPV status[J]. Am J Surg Pathol, 2008, 32(7):1044-1050.
doi: 10.1097/PAS.0b013e31816380ec |
| [23] |
Lai K, Killingsworth M, Matthews S, et al. Differences in survival outcome between oropharyngeal and oral cavity squamous cell carcinoma in relation to HPV status[J]. J Oral Pathol Med, 2017, 46(8):574-582.
doi: 10.1111/jop.2017.46.issue-8 |
| [24] |
Duncan LD, Winkler M, Carlson ER, et al. P16 immunohistochemistry can be used to detect human papillomavirus in oral cavity squamous cell carcinoma[J]. J Oral Maxillofac Surg, 2013, 71(8):1367-1375.
doi: 10.1016/j.joms.2013.02.019 |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Hao FU, Luyan SHEN, Bingyang HUANG, Shaohua MA. Clinical strategies for perioperative management of esophageal squamous cell carcinoma in the immunotherapy era [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 266-271. |
| [3] | Shang XIE, Luming WANG, Xinyuan ZHANG, Qiushi FENG, Yangyang XIA, Ziwei DAI, Xiaofeng SHAN, Zhigang CAI. Construction and application of oral squamous cell carcinoma organoid bank [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 847-851. |
| [4] | Minying MA, Xiaoqin CHAO, Yang ZHAO, Guoting ZHAO. Effects of LncRNA SNHG20 on epithelial mesenchymal transition and microtubule formation in human oral squamous cell carcinoma cells through targeted regulation of the miR-520c-3p/RAB22A pathway [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 26-32. |
| [5] | Li XU, Wen SHI, Yuehua LI, Yajun SHEN, Shang XIE, Xiaofeng SHAN, Zhigang CAI. LIM and calponin homology domains 1 may function as promising biological markers to aid in the prognostic prediction of oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 19-25. |
| [6] | Yaqing MAO, Zhen CHEN, Yao YU, Wenbo ZHANG, Yang LIU, Xin PENG. Impact of type 2 diabetes mellitus on the prognosis of patients with oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1089-1096. |
| [7] | Junqi SU,Xiaoying WANG,Zhiqiang SUN. Establishment and verification of a prognostic nomogram for survival of tongue squamous cell carcinoma patients who underwent cervical dissection [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 120-130. |
| [8] | Han LU,Jian-yun ZHANG,Rong YANG,Le XU,Qing-xiang LI,Yu-xing GUO,Chuan-bin GUO. Clinical factors affecting the prognosis of lower gingival squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 702-707. |
| [9] | SU Jun-qi,SONG Yang,XIE Shang. Analysis of etiological characteristics and establishment of prediction model of postoperative infections in patients undergoing oral squamous cell carcinoma surgery with free flap reconstruction [J]. Journal of Peking University (Health Sciences), 2022, 54(1): 68-76. |
| [10] | Lei-zhen SU,Jie CHEN,Xian LI,Ping JI. Effects of salinomycin on proliferation and apoptosis of oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2020, 52(5): 902-906. |
| [11] | Chuan-si-bo TAO,Fan DONG,Dian-can WANG,Chuan-bin GUO. Diagnostic test for detection of cervical lymph node metastasis from oral squamous cell carcinoma via infrared thermal imaging [J]. Journal of Peking University(Health Sciences), 2019, 51(5): 959-963. |
| [12] | Yang LIU,Yan GAO,Xue-jie CHEN,Hong HUA. DNA cytometry of exfoliated cells in the diagnosis of oral potential malignant disorders [J]. Journal of Peking University(Health Sciences), 2019, 51(1): 16-20. |
| [13] | Chun-feng ZHANG,Yun LIU,Min LU,Xiao-juan DU. Expression of hUTP14a in non-small cell lung cancer [J]. Journal of Peking University(Health Sciences), 2019, 51(1): 145-150. |
|
||