Journal of Peking University (Health Sciences) ›› 2023, Vol. 55 ›› Issue (1): 149-155. doi: 10.19723/j.issn.1671-167X.2023.01.023
Previous Articles Next Articles
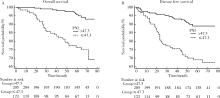
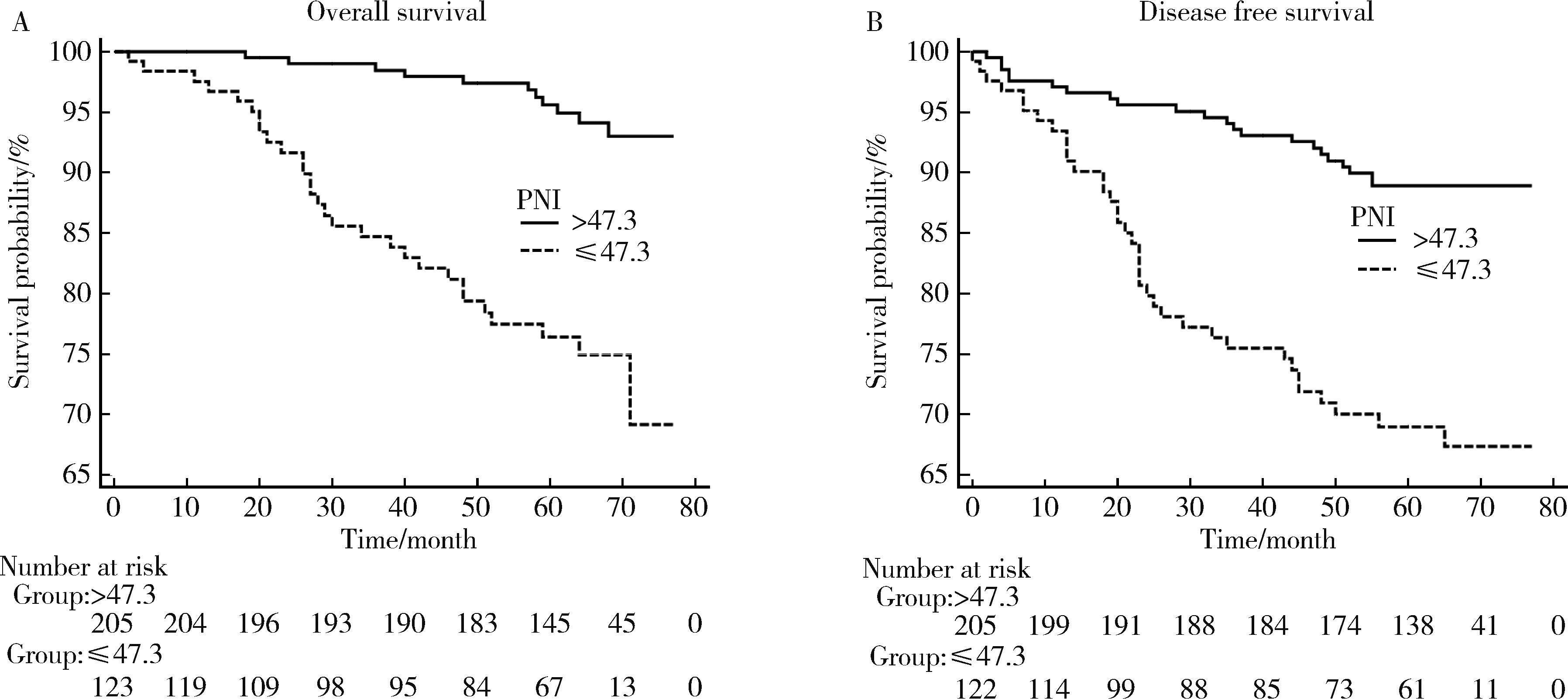
Pre-operative prognostic nutritional index as a predictive factor for prognosis in non-metastatic renal cell carcinoma treated with surgery
Quan ZHANG,Hai-feng SONG,Bing-lei MA,Zhe-nan ZHANG,Chao-hui ZHOU,Ao-lin LI,Jun LIU,Lei LIANG,Shi-yu ZHU,Qian ZHANG*( )
)
- Department of Urology, Peking University First Hospital; Institute of Urology, Peking University; National Urological Cancer Center, Beijing 100034, China
CLC Number:
- R737.11


| 1 |
Siegel RL , Miller KD , Jemal A . Cancer statistics, 2015[J]. CA Cancer J Clin, 2015, 65 (1): 5- 29.
doi: 10.3322/caac.21254 |
| 2 |
Janzen NK , Kim HL , Figlin RA , et al. Surveillance after radical or partial nephrectomy for localized renal cell carcinoma and management of recurrent disease[J]. Urol Clin North Am, 2003, 30 (4): 843- 852.
doi: 10.1016/S0094-0143(03)00056-9 |
| 3 |
Chrom P , Stec R , Bodnar L , et al. Incorporating neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in place of neutrophil count and platelet count improves prognostic accuracy of the International Metastatic Renal Cell Carcinoma Database Consortium model[J]. Cancer Res Treat, 2018, 50 (1): 103- 110.
doi: 10.4143/crt.2017.033 |
| 4 | Bazzi WM , Tin AL , Sjoberg DD , et al. The prognostic utility of preoperative neutrophil-to-lymphocyte ratio in localized clear cell renal cell carcinoma[J]. Can J Urol, 2016, 23 (1): 8151- 8154. |
| 5 | Hu K , Lou L , Ye J , et al. Prognostic role of the neutrophil-lymphocyte ratio in renal cell carcinoma: A meta-analysis[J]. BMJ Open, 2015, 5 (4): 6404- 6415. |
| 6 |
Jagdev SP , Gregory W , Vasudev NS , et al. Improving the accuracy of pre-operative survival prediction in renal cell carcinoma with C-reactive protein[J]. Br J Cancer, 2010, 103 (11): 1649- 1656.
doi: 10.1038/sj.bjc.6605973 |
| 7 | Onodera T , Goseki N , Kosaki G . Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients[J]. Nihon Geka Gakkai Zasshi, 1984, 85 (9): 1001- 1005. |
| 8 |
Borda A , Borda F , Vila J , et al. Predictive pre-treatment value of the prognostic nutritional index on survival in gastric carcinoma[J]. An Sist Sanit Navar, 2016, 39 (2): 227- 235.
doi: 10.23938/ASSN.0271 |
| 9 |
Nozoe T , Ninomiya M , Maeda T , et al. Prognostic nutritional index: A tool to predict the biological aggressiveness of gastric carcinoma[J]. Surg Today, 2010, 40 (5): 440- 443.
doi: 10.1007/s00595-009-4065-y |
| 10 |
Nozoe T , Kohno M , Iguchi T , et al. The prognostic nutritional index can be a prognostic indicator in colorectal carcinoma[J]. Surg Today, 2012, 42 (6): 532- 535.
doi: 10.1007/s00595-011-0061-0 |
| 11 |
Peng D , Gong YQ , Hao H , et al. Preoperative prognostic nutritional index is a significant predictor of survival with bladder cancer after radical cystectomy: A retrospective study[J]. BMC Cancer, 2017, 17 (1): 391- 399.
doi: 10.1186/s12885-017-3372-8 |
| 12 |
Xue W , Tan P , Xu H , et al. Impact of the preoperative prognostic nutritional index on survival outcomes in upper tract urothelial carcinomas[J]. Cancer Med, 2019, 8 (6): 2971- 2978.
doi: 10.1002/cam4.2161 |
| 13 | Cui J , Chen S , Bo Q , et al. Preoperative prognostic nutritional index and nomogram predicting recurrence-free survival in patients with primary non-muscle-invasive bladder cancer without carcinoma in situ[J]. Onco Targets Ther, 2017, 10 (1): 5541- 5550. |
| 14 |
Kang M , Chang CT , Sung HH , et al. Prognostic significance of pre- to postoperative dynamics of the prognostic nutritional index for patients with renal cell carcinoma who underwent radical nephrectomy[J]. Ann Surg Oncol, 2017, 24 (13): 4067- 4075.
doi: 10.1245/s10434-017-6065-2 |
| 15 |
Jeon HG , Choi DK , Sung HH , et al. Preoperative prognostic nutritional index is a significant predictor of survival in renal cell carcinoma patients undergoing nephrectomy[J]. Ann Surg Oncol, 2016, 23 (1): 321- 327.
doi: 10.1245/s10434-015-4614-0 |
| 16 |
Kang HW , Seo SP , Kim WT , et al. Low preoperative serum cholesterol level is associated with aggressive pathologic features and poor cancer-specific survival in patients with surgically treated renal cell carcinoma[J]. Int J Clin Oncol, 2018, 23 (1): 142- 150.
doi: 10.1007/s10147-017-1172-4 |
| 17 |
de Martino M , Leitner CV , Seemann C , et al. Preoperative serum cholesterol is an independent prognostic factor for patients with renal cell carcinoma (RCC)[J]. BJU Int, 2015, 115 (3): 397- 404.
doi: 10.1111/bju.12767 |
| 18 |
Chen Z , Shao Y , Wang K , et al. Prognostic role of pretreatment serum albumin in renal cell carcinoma: A systematic review and meta-analysis[J]. Onco Targets Ther, 2016, 9, 6701- 6710.
doi: 10.2147/OTT.S108469 |
| 19 | Byun SS , Hwang EC , Kang SH , et al. Prognostic significance of preoperative neutrophil-to-lymphocyte ratio in nonmetastatic renal cell carcinoma: A large, multicenter cohort analysis[J]. Biomed Res Int, 2016, 2016, 4148- 4156. |
| 20 | Grimes N , Hannan C , Tyson M , et al. The role of neutrophil-lymphocyte ratio as a prognostic indicator in patients undergoing nephrectomy for renal cell carcinoma[J]. Can Urol Assoc J, 2018, 12 (7): E345- E348. |
| 21 | Zhou W , Zhang GL . C-reactive protein to albumin ratio predicts the outcome in renal cell carcinoma: A meta-analysis[J]. PLoS One, 2019, 14 (10): 4266- 4277. |
| 22 |
Wang X , Su S , Guo Y . The clinical use of the platelet to lymphocyte ratio and lymphocyte to monocyte ratio as prognostic factors in renal cell carcinoma: A systematic review and meta-analysis[J]. Oncotarget, 2017, 8 (48): 84506- 84514.
doi: 10.18632/oncotarget.21108 |
| 23 |
Jiang N , Deng JY , Ding XW , et al. Prognostic nutritional index predicts postoperative complications and long-term outcomes of gastric cancer[J]. World J Gastroenterol, 2014, 20 (30): 10537- 10544.
doi: 10.3748/wjg.v20.i30.10537 |
| 24 |
Zheng Y , Bao L , Wang W , et al. Prognostic impact of the controlling nutritional status score following curative nephrectomy for patients with renal cell carcinoma[J]. Medicine (Baltimore), 2018, 97 (49): e13409.
doi: 10.1097/MD.0000000000013409 |
| 25 |
Kanda M , Mizuno A , Tanaka C , et al. Nutritional predictors for postoperative short-term and long-term outcomes of patients with gastric cancer[J]. Medicine (Baltimore), 2016, 95 (24): e3781.
doi: 10.1097/MD.0000000000003781 |
| 26 |
Song Y , Yang Y , Gao P , et al. The preoperative neutrophil to lymphocyte ratio is a superior indicator of prognosis compared with other inflammatory biomarkers in resectable colorectal cancer[J]. BMC Cancer, 2017, 17 (1): 391- 399.
doi: 10.1186/s12885-017-3372-8 |
| 27 |
Hu H , Yao X , Xie X , et al. Prognostic value of preoperative NLR, dNLR, PLR and CRP in surgical renal cell carcinoma patients[J]. World J Urol, 2017, 35 (2): 261- 270.
doi: 10.1007/s00345-016-1864-9 |
| 28 | Tsujino T , Komura K , Hashimoto T , et al. C-reactive protein-albumin ratio as a prognostic factor in renal cell carcinoma: A data from multi-institutional study in Japan[J]. Urol Oncol, 2019, 37 (11): 812.e1- 812.e8. |
| 29 |
Lien YC , Hsieh CC , Wu YC , et al. Preoperative serum albumin level is a prognostic indicator for adenocarcinoma of the gastric cardia[J]. J Gastrointest Surg, 2004, 8 (8): 1041- 1048.
doi: 10.1016/j.gassur.2004.09.033 |
| 30 |
Gupta D , Lis CG . Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature[J]. Nutr J, 2010, 9 (1): 69- 85.
doi: 10.1186/1475-2891-9-69 |
| 31 |
Chandra RK . Nutrition and immunology: From the clinic to cellular biology and back again[J]. Proc Nutr Soc, 1999, 58 (3): 681- 683.
doi: 10.1017/S0029665199000890 |
| 32 | Alwarawrah Y , Kiernan K , MacIver NJ . Changes in nutritional status impact immune cell metabolism and function[J]. Front Immunol, 2018, 9 (1): 1055- 1069. |
| 33 |
Tang Y , Liu Z , Liang J , et al. Early post-operative serum albumin level predicts survival after curative nephrectomy for kidney cancer: A retrospective study[J]. BMC Urol, 2018, 18 (1): 111- 118.
doi: 10.1186/s12894-018-0427-3 |
| 34 |
Corcoran AT , Kaffenberger SD , Clark PE , et al. Hypoalbuminaemia is associated with mortality in patients undergoing cytoreductive nephrectomy[J]. BJU Int, 2015, 116 (3): 351- 357.
doi: 10.1111/bju.12897 |
| 35 |
Stone PC , Lund S . Predicting prognosis in patients with advanced cancer[J]. Ann Oncol, 2007, 18 (6): 971- 976.
doi: 10.1093/annonc/mdl343 |
| 36 |
Volpe A , Patard JJ . Prognostic factors in renal cell carcinoma[J]. World J Urol, 2010, 28 (3): 319- 327.
doi: 10.1007/s00345-010-0540-8 |
| [1] | Junyong OU,Kunming NI,Lulin MA,Guoliang WANG,Ye YAN,Bin YANG,Gengwu LI,Haodong SONG,Min LU,Jianfei YE,Shudong ZHANG. Prognostic factors of patients with muscle invasive bladder cancer with intermediate-to-high risk prostate cancer [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 582-588. |
| [2] | Kewei CHEN,Zhuo LIU,Shaohui DENG,Fan ZHANG,Jianfei YE,Guoliang WANG,Shudong ZHANG. Clinical diagnosis and treatment of renal angiomyolipoma with inferior vena cava tumor thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 617-623. |
| [3] | Shuai LIU,Lei LIU,Zhuo LIU,Fan ZHANG,Lulin MA,Xiaojun TIAN,Xiaofei HOU,Guoliang WANG,Lei ZHAO,Shudong ZHANG. Clinical treatment and prognosis of adrenocortical carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 624-630. |
| [4] | Jie YANG,Jieli FENG,Shudong ZHANG,Lulin MA,Qing ZHENG. Clinical effects of transesophageal echocardiography in different surgical methods for nephrectomy combined with Mayo Ⅲ-Ⅳ vena tumor thrombectomy [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 631-635. |
| [5] | Le YU,Shaohui DENG,Fan ZHANG,Ye YAN,Jianfei YE,Shudong ZHANG. Clinicopathological characteristics and prognosis of multilocular cystic renal neoplasm of low malignant potential [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 661-666. |
| [6] | Fan SHU,Yichang HAO,Zhanyi ZHANG,Shaohui DENG,Hongxian ZHANG,Lei LIU,Guoliang WANG,Xiaojun TIAN,Lei ZHAO,Lulin MA,Shudong ZHANG. Functional and oncologic outcomes of partial nephrectomy for cystic renal cell carcinoma: A single-center retrospective study [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 667-672. |
| [7] | Zezhen ZHOU,Shaohui DENG,Ye YAN,Fan ZHANG,Yichang HAO,Liyuan GE,Hongxian ZHANG,Guoliang WANG,Shudong ZHANG. Predicting the 3-year tumor-specific survival in patients with T3a non-metastatic renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 673-679. |
| [8] | Yangyi FANG,Qiang LI,Zhigao HUANG,Min LU,Kai HONG,Shudong ZHANG. Well-differentiated papillary mesothelial tumour of the tunica vaginalis: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 741-744. |
| [9] | Yuanyuan ZENG,Yun XIE,Daonan CHEN,Ruilan WANG. Related factors of euthyroid sick syndrome in patients with sepsis [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 526-532. |
| [10] | Jian-bin LI,Meng-na LYU,Qiang CHI,Yi-lin PENG,Peng-cheng LIU,Rui WU. Early prediction of severe COVID-19 in patients with Sjögren’s syndrome [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1007-1012. |
| [11] | Yun-chong LIU,Zong-long WU,Li-yuan GE,Tan DU,Ya-qian WU,Yi-meng SONG,Cheng LIU,Lu-lin MA. Mechanism of nuclear protein 1 in the resistance to axitinib in clear cell renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 781-792. |
| [12] | Huan-rui LIU,Xiang PENG,Sen-lin LI,Xin GOU. Risk modeling based on HER-2 related genes for bladder cancer survival prognosis assessment [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 793-801. |
| [13] | Zi-xuan XUE,Shi-ying TANG,Min QIU,Cheng LIU,Xiao-jun TIAN,Min LU,Jing-han DONG,Lu-lin MA,Shu-dong ZHANG. Clinicopathologic features and prognosis of young renal tumors with tumor thrombus [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 802-811. |
| [14] | Dong LAN,Zhuo LIU,Yu-xuan LI,Guo-liang WANG,Xiao-jun TIAN,Lu-lin MA,Shu-dong ZHANG,Hong-xian ZHANG. Risk factors for massive hemorrhage after radical nephrectomy and removal of venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 825-832. |
| [15] | Min QIU,You-long ZONG,Bin-shuai WANG,Bin YANG,Chu-xiao XU,Zheng-hui SUN,Min LU,Lei ZHAO,Jian LU,Cheng LIU,Xiao-jun TIAN,Lu-lin MA. Treatment outcome of laparoscopic partial nephrectomy in patients with renal tumors of moderate to high complexity [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 833-837. |
|
||