Journal of Peking University (Health Sciences) ›› 2023, Vol. 55 ›› Issue (1): 149-155. doi: 10.19723/j.issn.1671-167X.2023.01.023
Previous Articles Next Articles
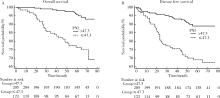
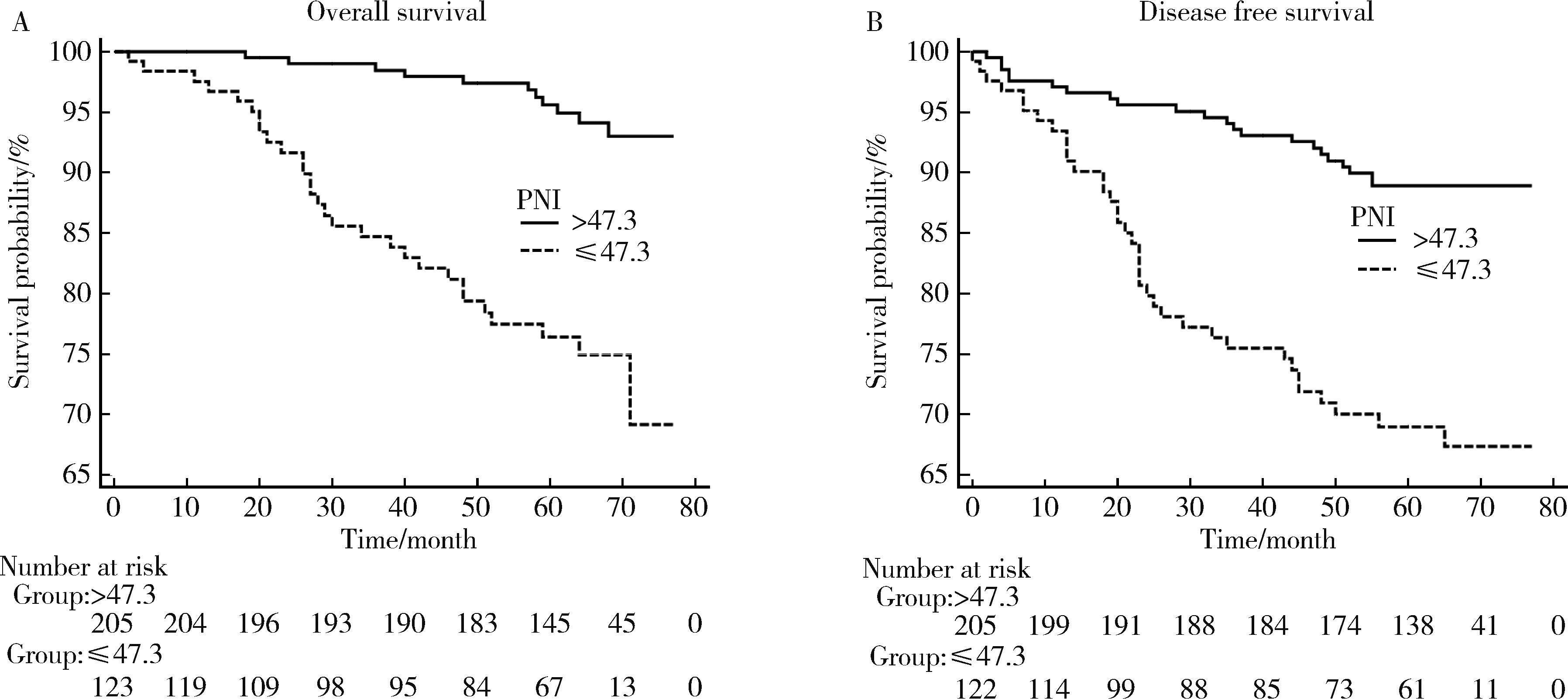
Pre-operative prognostic nutritional index as a predictive factor for prognosis in non-metastatic renal cell carcinoma treated with surgery
Quan ZHANG,Hai-feng SONG,Bing-lei MA,Zhe-nan ZHANG,Chao-hui ZHOU,Ao-lin LI,Jun LIU,Lei LIANG,Shi-yu ZHU,Qian ZHANG*( )
)
- Department of Urology, Peking University First Hospital; Institute of Urology, Peking University; National Urological Cancer Center, Beijing 100034, China
CLC Number:
- R737.11


| 1 |
Siegel RL , Miller KD , Jemal A . Cancer statistics, 2015[J]. CA Cancer J Clin, 2015, 65 (1): 5- 29.
doi: 10.3322/caac.21254 |
| 2 |
Janzen NK , Kim HL , Figlin RA , et al. Surveillance after radical or partial nephrectomy for localized renal cell carcinoma and management of recurrent disease[J]. Urol Clin North Am, 2003, 30 (4): 843- 852.
doi: 10.1016/S0094-0143(03)00056-9 |
| 3 |
Chrom P , Stec R , Bodnar L , et al. Incorporating neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in place of neutrophil count and platelet count improves prognostic accuracy of the International Metastatic Renal Cell Carcinoma Database Consortium model[J]. Cancer Res Treat, 2018, 50 (1): 103- 110.
doi: 10.4143/crt.2017.033 |
| 4 | Bazzi WM , Tin AL , Sjoberg DD , et al. The prognostic utility of preoperative neutrophil-to-lymphocyte ratio in localized clear cell renal cell carcinoma[J]. Can J Urol, 2016, 23 (1): 8151- 8154. |
| 5 | Hu K , Lou L , Ye J , et al. Prognostic role of the neutrophil-lymphocyte ratio in renal cell carcinoma: A meta-analysis[J]. BMJ Open, 2015, 5 (4): 6404- 6415. |
| 6 |
Jagdev SP , Gregory W , Vasudev NS , et al. Improving the accuracy of pre-operative survival prediction in renal cell carcinoma with C-reactive protein[J]. Br J Cancer, 2010, 103 (11): 1649- 1656.
doi: 10.1038/sj.bjc.6605973 |
| 7 | Onodera T , Goseki N , Kosaki G . Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients[J]. Nihon Geka Gakkai Zasshi, 1984, 85 (9): 1001- 1005. |
| 8 |
Borda A , Borda F , Vila J , et al. Predictive pre-treatment value of the prognostic nutritional index on survival in gastric carcinoma[J]. An Sist Sanit Navar, 2016, 39 (2): 227- 235.
doi: 10.23938/ASSN.0271 |
| 9 |
Nozoe T , Ninomiya M , Maeda T , et al. Prognostic nutritional index: A tool to predict the biological aggressiveness of gastric carcinoma[J]. Surg Today, 2010, 40 (5): 440- 443.
doi: 10.1007/s00595-009-4065-y |
| 10 |
Nozoe T , Kohno M , Iguchi T , et al. The prognostic nutritional index can be a prognostic indicator in colorectal carcinoma[J]. Surg Today, 2012, 42 (6): 532- 535.
doi: 10.1007/s00595-011-0061-0 |
| 11 |
Peng D , Gong YQ , Hao H , et al. Preoperative prognostic nutritional index is a significant predictor of survival with bladder cancer after radical cystectomy: A retrospective study[J]. BMC Cancer, 2017, 17 (1): 391- 399.
doi: 10.1186/s12885-017-3372-8 |
| 12 |
Xue W , Tan P , Xu H , et al. Impact of the preoperative prognostic nutritional index on survival outcomes in upper tract urothelial carcinomas[J]. Cancer Med, 2019, 8 (6): 2971- 2978.
doi: 10.1002/cam4.2161 |
| 13 | Cui J , Chen S , Bo Q , et al. Preoperative prognostic nutritional index and nomogram predicting recurrence-free survival in patients with primary non-muscle-invasive bladder cancer without carcinoma in situ[J]. Onco Targets Ther, 2017, 10 (1): 5541- 5550. |
| 14 |
Kang M , Chang CT , Sung HH , et al. Prognostic significance of pre- to postoperative dynamics of the prognostic nutritional index for patients with renal cell carcinoma who underwent radical nephrectomy[J]. Ann Surg Oncol, 2017, 24 (13): 4067- 4075.
doi: 10.1245/s10434-017-6065-2 |
| 15 |
Jeon HG , Choi DK , Sung HH , et al. Preoperative prognostic nutritional index is a significant predictor of survival in renal cell carcinoma patients undergoing nephrectomy[J]. Ann Surg Oncol, 2016, 23 (1): 321- 327.
doi: 10.1245/s10434-015-4614-0 |
| 16 |
Kang HW , Seo SP , Kim WT , et al. Low preoperative serum cholesterol level is associated with aggressive pathologic features and poor cancer-specific survival in patients with surgically treated renal cell carcinoma[J]. Int J Clin Oncol, 2018, 23 (1): 142- 150.
doi: 10.1007/s10147-017-1172-4 |
| 17 |
de Martino M , Leitner CV , Seemann C , et al. Preoperative serum cholesterol is an independent prognostic factor for patients with renal cell carcinoma (RCC)[J]. BJU Int, 2015, 115 (3): 397- 404.
doi: 10.1111/bju.12767 |
| 18 |
Chen Z , Shao Y , Wang K , et al. Prognostic role of pretreatment serum albumin in renal cell carcinoma: A systematic review and meta-analysis[J]. Onco Targets Ther, 2016, 9, 6701- 6710.
doi: 10.2147/OTT.S108469 |
| 19 | Byun SS , Hwang EC , Kang SH , et al. Prognostic significance of preoperative neutrophil-to-lymphocyte ratio in nonmetastatic renal cell carcinoma: A large, multicenter cohort analysis[J]. Biomed Res Int, 2016, 2016, 4148- 4156. |
| 20 | Grimes N , Hannan C , Tyson M , et al. The role of neutrophil-lymphocyte ratio as a prognostic indicator in patients undergoing nephrectomy for renal cell carcinoma[J]. Can Urol Assoc J, 2018, 12 (7): E345- E348. |
| 21 | Zhou W , Zhang GL . C-reactive protein to albumin ratio predicts the outcome in renal cell carcinoma: A meta-analysis[J]. PLoS One, 2019, 14 (10): 4266- 4277. |
| 22 |
Wang X , Su S , Guo Y . The clinical use of the platelet to lymphocyte ratio and lymphocyte to monocyte ratio as prognostic factors in renal cell carcinoma: A systematic review and meta-analysis[J]. Oncotarget, 2017, 8 (48): 84506- 84514.
doi: 10.18632/oncotarget.21108 |
| 23 |
Jiang N , Deng JY , Ding XW , et al. Prognostic nutritional index predicts postoperative complications and long-term outcomes of gastric cancer[J]. World J Gastroenterol, 2014, 20 (30): 10537- 10544.
doi: 10.3748/wjg.v20.i30.10537 |
| 24 |
Zheng Y , Bao L , Wang W , et al. Prognostic impact of the controlling nutritional status score following curative nephrectomy for patients with renal cell carcinoma[J]. Medicine (Baltimore), 2018, 97 (49): e13409.
doi: 10.1097/MD.0000000000013409 |
| 25 |
Kanda M , Mizuno A , Tanaka C , et al. Nutritional predictors for postoperative short-term and long-term outcomes of patients with gastric cancer[J]. Medicine (Baltimore), 2016, 95 (24): e3781.
doi: 10.1097/MD.0000000000003781 |
| 26 |
Song Y , Yang Y , Gao P , et al. The preoperative neutrophil to lymphocyte ratio is a superior indicator of prognosis compared with other inflammatory biomarkers in resectable colorectal cancer[J]. BMC Cancer, 2017, 17 (1): 391- 399.
doi: 10.1186/s12885-017-3372-8 |
| 27 |
Hu H , Yao X , Xie X , et al. Prognostic value of preoperative NLR, dNLR, PLR and CRP in surgical renal cell carcinoma patients[J]. World J Urol, 2017, 35 (2): 261- 270.
doi: 10.1007/s00345-016-1864-9 |
| 28 | Tsujino T , Komura K , Hashimoto T , et al. C-reactive protein-albumin ratio as a prognostic factor in renal cell carcinoma: A data from multi-institutional study in Japan[J]. Urol Oncol, 2019, 37 (11): 812.e1- 812.e8. |
| 29 |
Lien YC , Hsieh CC , Wu YC , et al. Preoperative serum albumin level is a prognostic indicator for adenocarcinoma of the gastric cardia[J]. J Gastrointest Surg, 2004, 8 (8): 1041- 1048.
doi: 10.1016/j.gassur.2004.09.033 |
| 30 |
Gupta D , Lis CG . Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature[J]. Nutr J, 2010, 9 (1): 69- 85.
doi: 10.1186/1475-2891-9-69 |
| 31 |
Chandra RK . Nutrition and immunology: From the clinic to cellular biology and back again[J]. Proc Nutr Soc, 1999, 58 (3): 681- 683.
doi: 10.1017/S0029665199000890 |
| 32 | Alwarawrah Y , Kiernan K , MacIver NJ . Changes in nutritional status impact immune cell metabolism and function[J]. Front Immunol, 2018, 9 (1): 1055- 1069. |
| 33 |
Tang Y , Liu Z , Liang J , et al. Early post-operative serum albumin level predicts survival after curative nephrectomy for kidney cancer: A retrospective study[J]. BMC Urol, 2018, 18 (1): 111- 118.
doi: 10.1186/s12894-018-0427-3 |
| 34 |
Corcoran AT , Kaffenberger SD , Clark PE , et al. Hypoalbuminaemia is associated with mortality in patients undergoing cytoreductive nephrectomy[J]. BJU Int, 2015, 116 (3): 351- 357.
doi: 10.1111/bju.12897 |
| 35 |
Stone PC , Lund S . Predicting prognosis in patients with advanced cancer[J]. Ann Oncol, 2007, 18 (6): 971- 976.
doi: 10.1093/annonc/mdl343 |
| 36 |
Volpe A , Patard JJ . Prognostic factors in renal cell carcinoma[J]. World J Urol, 2010, 28 (3): 319- 327.
doi: 10.1007/s00345-010-0540-8 |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Fan SHU, Liyuan GE, Hanzhang DENG, Haoming YIN, Junyong OU, Shaohui DENG, Yichang HAO, Min LU, Zhanyi ZHANG, Peichen DUAN, Shudong ZHANG. Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 631-640. |
| [3] | Haoming YIN, Zijie WANG, Fan SHU, Zhanyi ZHANG, Hui LIANG, Shudong ZHANG. Expression and significance of the FABP6 long transcript in clear cell renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 393-398. |
| [4] | Lingfu ZHANG, Ming CHEN, Xiaoyu ZHAO, Gang WANG, Long CUI, Xiaofeng LING, Lixin WANG, Zhi XU, Limei GUO, Chunsheng HOU. Gross classification of gallbladder cancer with primary lesion limited to the gallbladder wall and its correlation with prognosis and precancerous lesions [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 184-189. |
| [5] | Boda GUO, Min LU, Guoliang WANG, Hongxian ZHANG, Lei LIU, Xiaofei HOU, Lei ZHAO, Xiaojun TIAN, Shudong ZHANG. Clinicopathological and prognostic differences between clear cell and non-clear cell renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 644-649. |
| [6] | Zhanyi ZHANG, Min LU, Yuehao SUN, Jinghan DONG, Xiaofei HOU, Chunlei XIAO, Guoliang WANG, Xiaojun TIAN, Lulin MA, Hongxian ZHANG, Shudong ZHANG. Clinicopathological features and survival analysis of TFE3-rearranged renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 650-661. |
| [7] | Qiming ZHANG, Zebo CHEN, Yu TIAN, Dameng PAN, Lei LIU, Hongxian ZHANG, Lei ZHAO, Shudong ZHANG, Lulin MA, Xiaofei HOU. Experience summary of robot-assisted laparoscopic transplant nephrectomy [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 666-669. |
| [8] | Zezhen ZHOU, Liyuan GE, Fan ZHANG, Shaohui DENG, Ye YAN, Hongxian ZHANG, Guoliang WANG, Lei LIU, Yi HUANG, Shudong ZHANG. A retrospective matching study of partial nephrectomy and radical nephrectomy for pathological T3a stage renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 704-710. |
| [9] | Weihao LI, Jing LI, Xuemin ZHANG, Wei LI, Qingle LI, Xiaoming ZHANG. Effect of intraoperative blood salvage autotransfusion on the prognosis of patients after carotid body tumor resection [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 272-276. |
| [10] | Yaqing MAO, Zhen CHEN, Yao YU, Wenbo ZHANG, Yang LIU, Xin PENG. Impact of type 2 diabetes mellitus on the prognosis of patients with oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1089-1096. |
| [11] | Junyong OU,Kunming NI,Lulin MA,Guoliang WANG,Ye YAN,Bin YANG,Gengwu LI,Haodong SONG,Min LU,Jianfei YE,Shudong ZHANG. Prognostic factors of patients with muscle invasive bladder cancer with intermediate-to-high risk prostate cancer [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 582-588. |
| [12] | Kewei CHEN,Zhuo LIU,Shaohui DENG,Fan ZHANG,Jianfei YE,Guoliang WANG,Shudong ZHANG. Clinical diagnosis and treatment of renal angiomyolipoma with inferior vena cava tumor thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 617-623. |
| [13] | Shuai LIU,Lei LIU,Zhuo LIU,Fan ZHANG,Lulin MA,Xiaojun TIAN,Xiaofei HOU,Guoliang WANG,Lei ZHAO,Shudong ZHANG. Clinical treatment and prognosis of adrenocortical carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 624-630. |
| [14] | Jie YANG,Jieli FENG,Shudong ZHANG,Lulin MA,Qing ZHENG. Clinical effects of transesophageal echocardiography in different surgical methods for nephrectomy combined with Mayo Ⅲ-Ⅳ vena tumor thrombectomy [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 631-635. |
| [15] | Le YU,Shaohui DENG,Fan ZHANG,Ye YAN,Jianfei YE,Shudong ZHANG. Clinicopathological characteristics and prognosis of multilocular cystic renal neoplasm of low malignant potential [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 661-666. |
|
||