Journal of Peking University (Health Sciences) ›› 2025, Vol. 57 ›› Issue (3): 537-544. doi: 10.19723/j.issn.1671-167X.2025.03.018
Previous Articles Next Articles
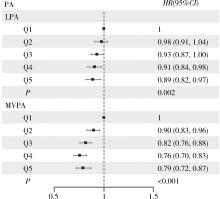
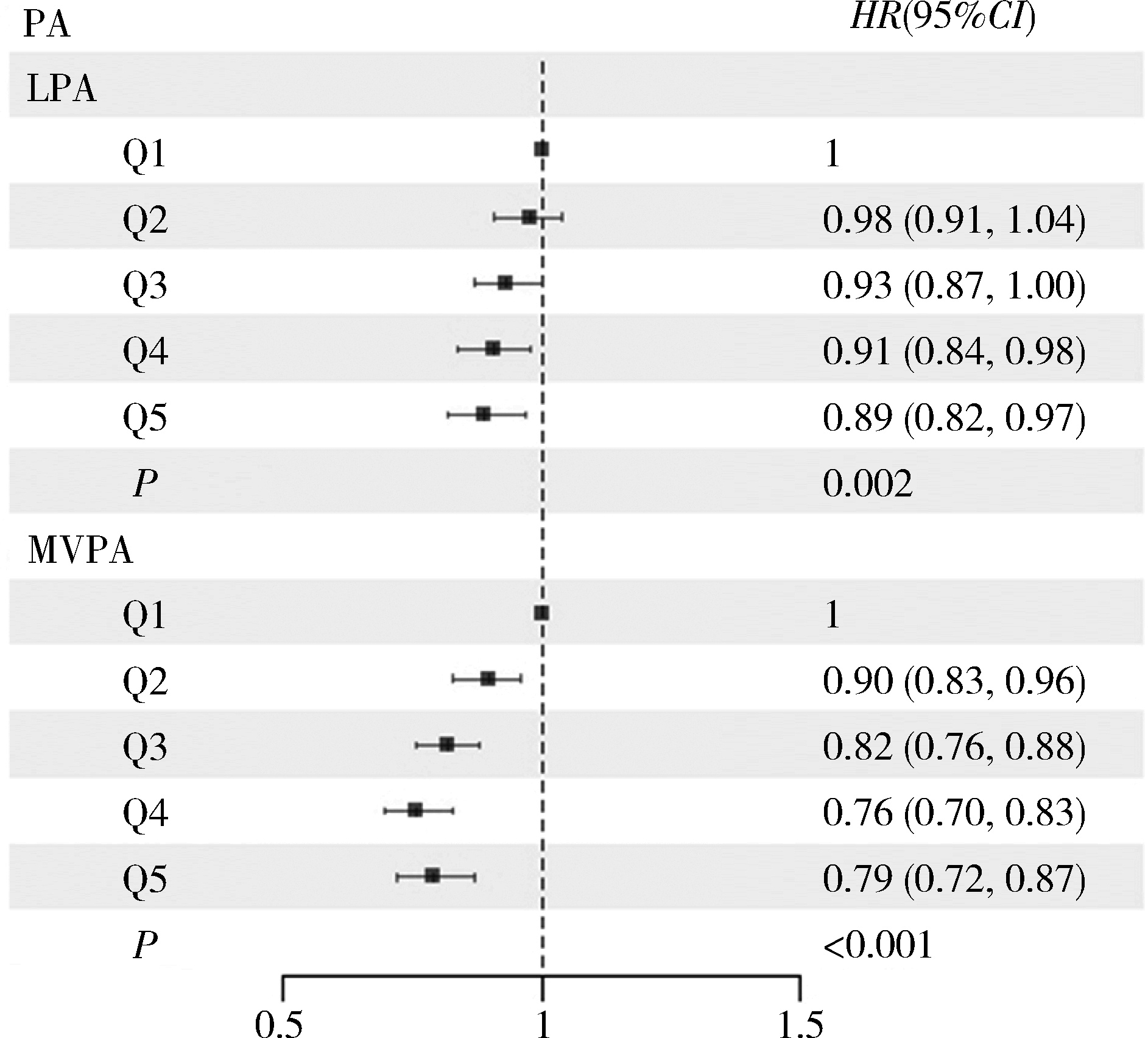
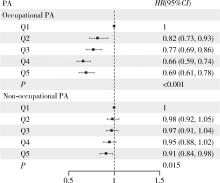
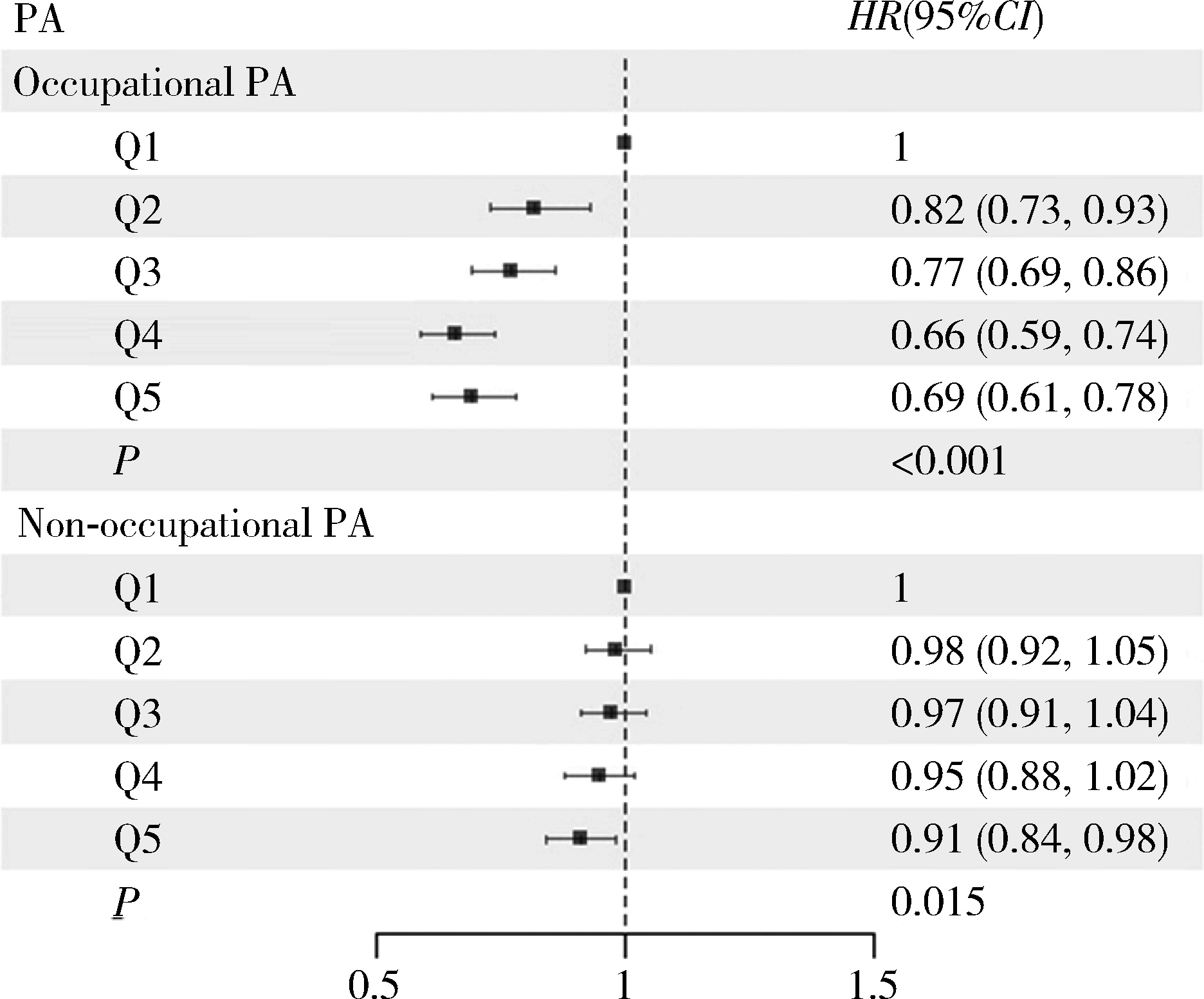
Prospective association between physical activity and mortality in patients with chronic obstructive pulmonary disease
Shuo ZHANG1, Yongbing LAN1, Dianjianyi SUN1,2,3, Pei PEI2, Huaidong DU4, Junshi CHEN5, Zhengming CHEN4, Jun LV1,2,3,6, Liming LI1,2,3, Canqing YU1,2,3,*( ), (for the China Kadoorie Biobank Collaborative Group)
), (for the China Kadoorie Biobank Collaborative Group)
- 1. Department of Epidemiology & Biostatistics, Peking University School of Public Health, Beijing 100191, China
2. Peking University Center for Public Health and Epidemic Preparedness & Response, Beijing 100191, China
3. Key Laboratory of Epidemiology of Major Diseases (Peking University), Ministry of Education, Beijing 100191, China
4. Clinical Trial Service Unit and Epidemiological Studies Unit, Nuffield Department of Population Health, University of Oxford, Oxford OX3 7LF, UK
5. China National Center for Food Safety Risk Assessment, Beijing 100022, China
6. State Key Laboratory of Vascular Homeostasis and Remodeling, Peking University, Beijing 100191, China
CLC Number:
- R184
| 1 |
慢性阻塞性肺疾病急性加重诊治专家组. 慢性阻塞性肺疾病急性加重诊治中国专家共识[J]. 国际呼吸杂志, 2023, 43 (2): 132- 149.
|
| 2 |
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2025 update[EB/OL]. (2025-01-01)[2025-01-15]. https://www.goldcopd.org.
|
| 3 |
doi: 10.1016/S0140-6736(18)30841-9 |
| 4 |
doi: 10.1164/rccm.200612-1749OC |
| 5 |
doi: 10.1016/S2214-109X(23)00217-6 |
| 6 |
World Health Organization. WHO guidelines on physical activity and sedentary behaviour [EB/OL]. (2020-11-25)[2024-12-25]. https://www.who.int/publications/i/item/9789240015128.
|
| 7 |
doi: 10.1016/S0140-6736(17)31222-9 |
| 8 |
doi: 10.1093/ije/dyr120 |
| 9 |
doi: 10.1093/ije/dyi174 |
| 10 |
doi: 10.1249/MSS.0b013e31821ece12 |
| 11 |
樊萌语, 吕筠, 郭彧, 等. 中国慢性病前瞻性研究: 10个项目地区成人体力活动和休闲静坐时间特征差异的分析[J]. 中华流行病学杂志, 2015, 36 (8): 779- 785.
|
| 12 |
中华人民共和国国家卫生健康委员会医政司. 肥胖症诊疗指南(2024年版)[J]. 中华消化外科杂志, 2024, 23 (10): 1237- 1260.
doi: 10.3760/cma.j.cn115610-20241017-00455 |
| 13 |
doi: 10.1186/s12889-018-5167-5 |
| 14 |
孙明希, 温启邦, 涂华康, 等. 4种慢性病共病模式及运动与全因死亡的相关性研究[J]. 中华流行病学杂志, 2022, 43 (12): 1952- 1958.
|
| 15 |
doi: 10.1378/chest.10-2521 |
| 16 |
doi: 10.1378/chest.11-2014 |
| 17 |
doi: 10.1016/j.chest.2023.07.017 |
| 18 |
|
| 19 |
doi: 10.1097/PHM.0000000000002612 |
| 20 |
doi: 10.1080/17461391.2019.1697375 |
| 21 |
|
| 22 |
|
| 23 |
|
| 24 |
|
| 25 |
|
| 26 |
|
| 27 |
Hu YZ, Sun QF, Han YT, et al. Role of lifestyle factors on the development and long-term prognosis of pneumonia and cardiovascular disease in the Chinese population[J]. Chin Med J (Engl), 2024, 8 (2024-08-28)[2024-12-26]. https://pubmed.ncbi.nlm.nih.gov/39193696.
|
| [1] | Chang LIU, Zhao LI, Lei JIN, Chunyi LIU, Chunjing WANG, Jie ZHANG, Lei JIN. Association between maternal periconceptional supplementation of folic acid or multiple micronutrients containing folic acid and perinatal mortality rate [J]. Journal of Peking University (Health Sciences), 2025, 57(3): 473-480. |
| [2] | Yuxin WANG, Ru CAO, Jing HUANG, Ponsawansong Pitakchon, Tawatsupa Benjawan, Xiaochuan PAN, Prapamontol Tippawan, Guoxing LI. Impact of fine particulate matter exposure on non-accidental mortality under different apparent temperature levels [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 820-827. |
| [3] | Qingxin ZHOU,Qingqing YANG,Shuyuan SHI,Pei LI,Feng SUN. Association between serum uric acid and airflow obstruction based on the health-checkup population [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 693-699. |
| [4] | Shan CAI,Yihang ZHANG,Ziyue CHEN,Yunfe LIU,Jiajia DANG,Di SHI,Jiaxin LI,Tianyu HUANG,Jun MA,Yi SONG. Status and pathways of factors influencing physical activity time among elementary and junior high school students in Beijing [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 403-410. |
| [5] | Zi-kai WANG,Jia-li MO,Meng ZHANG,Ji-ping LIAO. Epidemiology and hospitalization costs analysis of female inpatients with acute exacerbation of chronic obstructive pulmonary disease in Beijing from 2013 to 2020 [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1074-1081. |
| [6] | Ya-nan ZHAO,Hui-yun FAN,Xiang-yu WANG,Ya-nan LUO,Rong ZHANG,Xiao-ying ZHENG. Early death and causes of death of patients with autism spectrum disorders: A systematic review [J]. Journal of Peking University (Health Sciences), 2023, 55(2): 375-383. |
| [7] | Yun-fei LIU,Jia-jia DANG,Pan-liang ZHONG,Ning MA,Di SHI,Yi SONG. Injury mortality among Chinese aged 5 to 24 years from 1990 to 2019 [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 498-504. |
| [8] | Yi-hua LIU,Qing-ping YUN,Lan-chao ZHANG,Xiao-yue ZHANG,Yu-ting LIN,Fang-jing LIU,Zhi-jie ZHENG,Chun CHANG. Joint association of sedentary behavior and physical activity on anxiety tendency among occupational population in China [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 490-497. |
| [9] | LIU Jie,GUO Chao. A prospective cohort study of the influence of positive/negative effectivity on the mortality risk of the Chinese elderly [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 255-260. |
| [10] | Xiao-na NA,Zhu ZHU,Yang-yang CHEN,Dong-ping WANG,Hao-jie WANG,Yang SONG,Xiao-chuan MA,Pei-yu WANG,Ai-ping LIU. Associations of distribution of time spent in physical activity and sedentary behavior with obesity [J]. Journal of Peking University (Health Sciences), 2020, 52(3): 486-491. |
| [11] | Yi SONG,Dong-mei LUO,Pei-jin HU,Xiao-jin YAN,Jing-shu ZHANG,Yuan-ting LEI,Bing ZHANG,Jun MA. Trends of prevalence of excellent health status and physical fitness among Chinese Han students aged 13 to 18 years from 1985 to 2014 [J]. Journal of Peking University (Health Sciences), 2020, 52(2): 317-322. |
| [12] | Hai-rong BAO,Xiao-ju LIU,En-li TAN,Juan SHU,Ji-yuan DONG,Sheng LI. Effects of temperature and relative humidity on the number of outpatients with chronic obstructive pulmonary disease and their interaction effect in Lanzhou, China [J]. Journal of Peking University (Health Sciences), 2020, 52(2): 308-316. |
| [13] | Wen TANG,Jun-yi GAO,Xin-yu MA,Chao-he ZHANG,Lian-tao MA,Ya-sha WANG. Application of recurrent neural network in prognosis of peritoneal dialysis [J]. Journal of Peking University(Health Sciences), 2019, 51(3): 602-608. |
| [14] | Jiang XIE,Fei LI. Association of sleep overlap syndrome with type 2 diabetes in a cross-sectional study [J]. Journal of Peking University(Health Sciences), 2019, 51(2): 252-255. |
| [15] | WU Shi-yan1, ZHANG Xu-xi1, SUN Kai-ge1, HU Kang, LIU Si-jia, SUN Xin-ying. Application of multi-group structural equation model in comparative study of HBM related to recreational physical activity among population with high risk of chronic diseases and healthy people [J]. Journal of Peking University(Health Sciences), 2018, 50(4): 711-716. |
|
||