Journal of Peking University (Health Sciences) ›› 2025, Vol. 57 ›› Issue (5): 947-955. doi: 10.19723/j.issn.1671-167X.2025.05.020
Previous Articles Next Articles
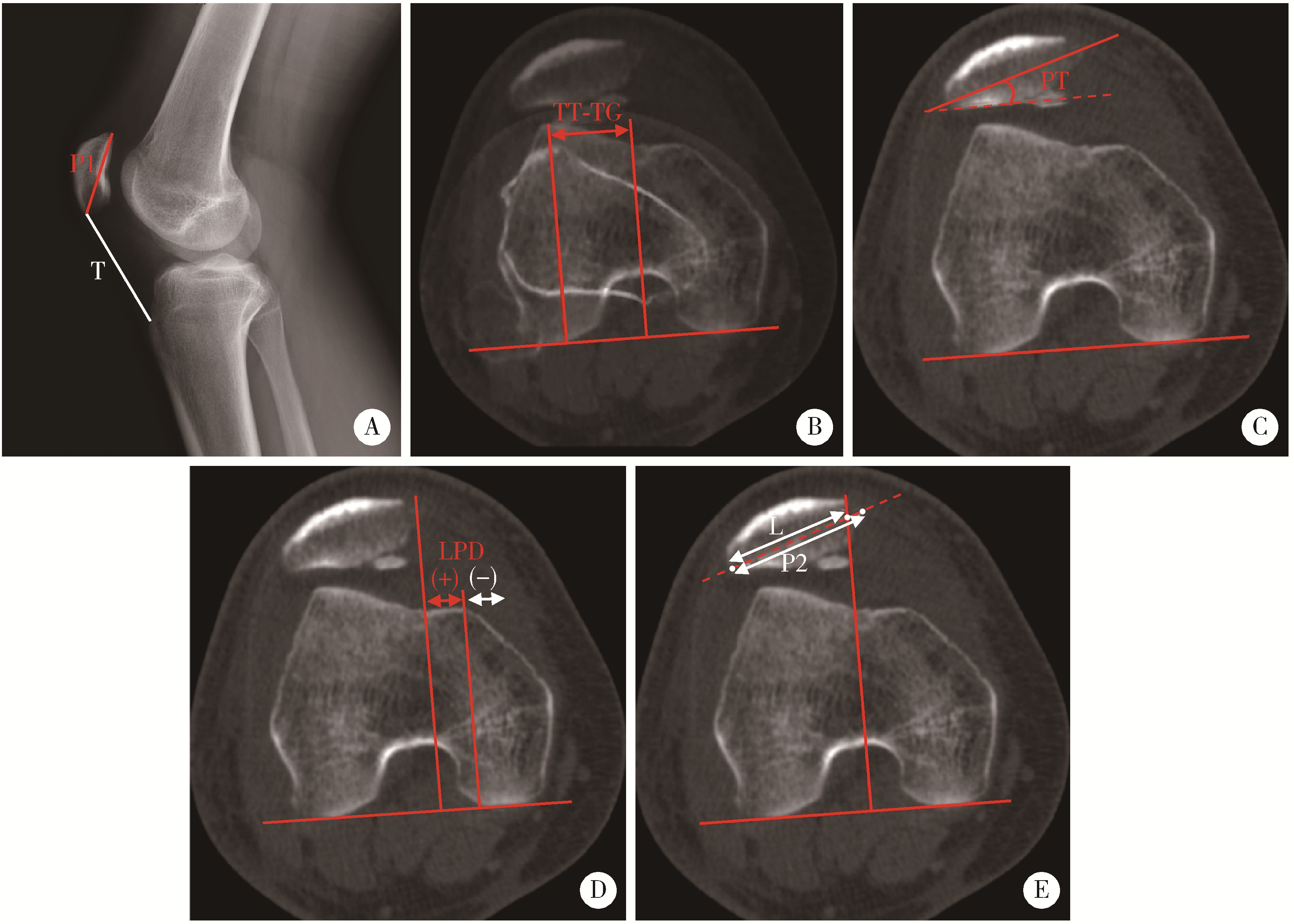
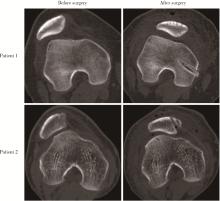
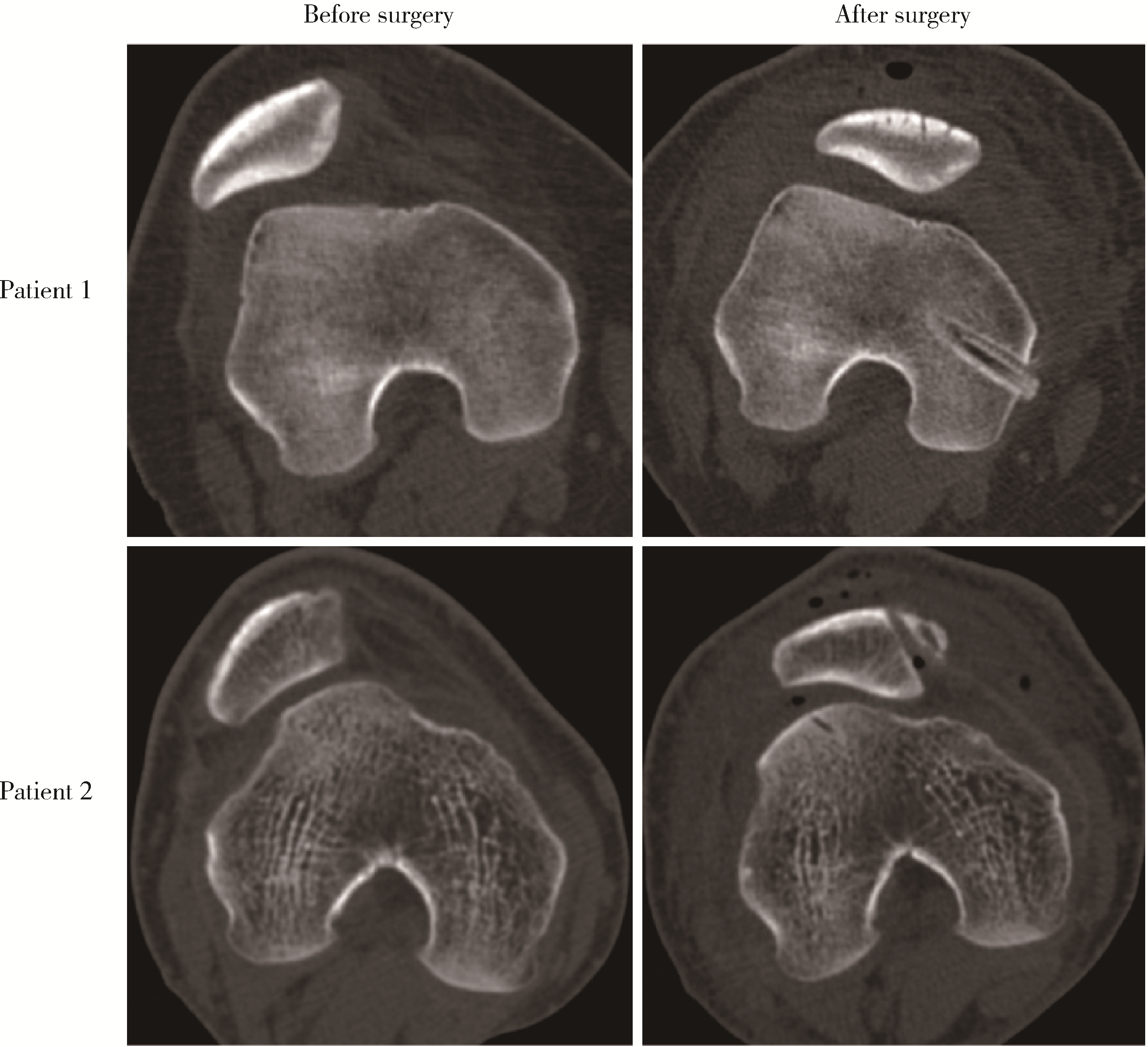
Clinical efficacy of arthroscopic medial patellofemoral complex reconstruction for recurrent patellar dislocation with high-grade trochlear dysplasia
Fengyi HU, Qingyang MENG, Nayun CHEN, Jianing WANG, Zhenlong LIU, Yong MA, Yuping YANG, Xi GONG, Cheng WANG, Ping LIU*( ), Weili SHI*()
), Weili SHI*()
- Department of Sports Medicine, Peking University Third Hospital; Institute of Sports Medicine of Peking University; Beijing Key Laboratory of Sports Injuries, Beijing 100191, China
CLC Number:
- R684.76

| 1 |
doi: 10.1177/1941738117725055 |
| 2 |
doi: 10.1177/0363546517732045 |
| 3 |
doi: 10.1007/s00167-004-0607-4 |
| 4 |
doi: 10.1016/j.eats.2013.01.002 |
| 5 |
doi: 10.2106/JBJS.15.01182 |
| 6 |
doi: 10.1007/s00167-020-05999-2 |
| 7 |
doi: 10.1016/j.arthro.2020.01.058 |
| 8 |
印钰, 陈临新, 梅宇, 等. 内侧股四头肌腱股骨韧带重建联合单骨道内侧髌股韧带重建治疗复发性髌骨脱位的临床疗效[J]. 中国运动医学杂志, 2021, 40 (12): 936- 941.
|
| 9 |
doi: 10.1097/BPO.0000000000001259 |
| 10 |
doi: 10.1016/j.eats.2020.09.026 |
| 11 |
doi: 10.1016/j.eats.2019.01.006 |
| 12 |
doi: 10.1177/0363546516635626 |
| 13 |
doi: 10.1177/0363546515606102 |
| 14 |
doi: 10.1177/0363546520958423 |
| 15 |
doi: 10.1177/0363546517745625 |
| 16 |
doi: 10.1016/j.arthro.2022.06.038 |
| 17 |
|
| 18 |
doi: 10.2214/AJR.19.22400 |
| 19 |
doi: 10.1186/s12891-019-2697-7 |
| 20 |
doi: 10.1177/0363546520916435 |
| 21 |
doi: 10.1097/JSA.0000000000000252 |
| 22 |
doi: 10.1007/s00167-018-5266-y |
| 23 |
doi: 10.1177/0363546515572143 |
| 24 |
doi: 10.1177/03635465211041087 |
| 25 |
doi: 10.1177/0363546519838405 |
| 26 |
doi: 10.1177/0363546513518413 |
| 27 |
doi: 10.1007/s00167-015-3698-1 |
| 28 |
doi: 10.1016/j.arthro.2022.04.019 |
| 29 |
doi: 10.1177/0363546519835800 |
| [1] | Yujing ZHU, Lei WANG, Chengyin LYU, Wenfeng TAN, Miaojia ZHANG. Analysis of clinical features of ruccrent interstitial lung disease in patients with anti-EJ positive antisynthetase syndrome [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 980-986. |
| [2] | Yukai LI, Hongyan WANG, Liang LUO, Yun LI, Chun LI. Clinical significance of antiphospholipid antibodies in Behcet disease with thrombosis [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1036-1040. |
| [3] | Yuqing LI,Biao WANG,Peng QIAO,Wei WANG,Xing GUAN. Medium to long-term efficacy of tension-free vaginal tape procedure in the treatment of female recurrent stress urinary incontinence [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 600-604. |
| [4] | Chieko MORIMOTO,Yi-qin WANG,Rong ZHOU,Jian-liu WANG. Clinical analysis of fertility-sparing therapy of patients with complex atypical hyperplasia and endometrial cancer [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 936-942. |
| [5] | Yue WANG,Shuang ZHANG,Hong ZHANG,Li LIANG,Ling XU,Yuan-jia CHENG,Xue-ning DUAN,Yin-hua LIU,Ting LI. Clinicopathological features and prognosis of hormone receptor-positive/human epidermal growth factor receptor 2-negative breast cancer [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 853-862. |
| [6] | Su-hua CHEN,Jun YANG,Xin CHEN,Chen-long YANG,Jian-jun SUN,Guo-zhong LIN,Tao YU,Xin YANG,Yun-feng HAN,Chao WU,Yu SI,Kai-ming MA. Surgical treatment of large and giant recurrent meningiomas near the middle and posterior third part of the superior sagittal sinus with extracranial invading [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 1006-1012. |
| [7] | LIU Lei,QIN Yan-chun,WANG Guo-liang,ZHANG Shu-dong,HOU Xiao-fei,MA Lu-lin. Strategy of reoperation for pheochromocytoma and paraganglioma [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 793-797. |
| [8] | Huan-bin YU,Wen-jie WU,Xiao-ming LV,Yan SHI,Lei ZHENG,Jian-guo ZHANG. 125I seed brachytherapy for recurrent salivary gland carcinoma after external radiotherapy [J]. Journal of Peking University (Health Sciences), 2020, 52(5): 919-923. |
| [9] | Xu-chu ZHANG,Jian-hua ZHANG,Rong-fu WANG,Yan FAN,Zhan-li FU,Ping YAN,Guang-yu ZHAO,Yan-xia BAI. Diagnostic value of 18F-FDG PET/CT and tumor markers (CEA, CA19-9, CA24-2) in recurrence and metastasis of postoperative colorectal moderately differentiated adenocarcinoma [J]. Journal of Peking University(Health Sciences), 2019, 51(6): 1071-1077. |
| [10] | Qi TANG,Rong-cheng LIN,Lin YAO,Zheng ZHANG,Han HAO,Cui-jian ZHANG,Lin CAI,Xue-song LI,Zhi-song HE,Li-qun ZHOU. Clinicopathologic features and prognostic analyses of locally recurrent renal cell carcinoma patients after initial surgery [J]. Journal of Peking University(Health Sciences), 2019, 51(4): 628-631. |
| [11] | XING Yun-chao, XIONG Geng-yan, FANG Dong, ZHANG Zheng, CAI Lin, ZHANG Lei, HE Zhi-song, LI Xue-song, ZHOU Li-qun. Preoperative prognostic factors and preoperative risk stratification of upper tract urothelial carcinoma [J]. Journal of Peking University(Health Sciences), 2016, 48(6): 1032-1037. |
| [12] | LIU Yu-Qing, LU Jian, ZHAO Lei, HOU Xiao-Fei, MA Lu-Lin. Prognostic factors for intravesical recurrence after surgery for upper tract urothelial carcinoma in renal transplant recipients [J]. Journal of Peking University(Health Sciences), 2015, 47(4): 605-610. |
| [13] | YANG Yang, XIAO Yun-Xiang, ZHOU Li-Qun, HE Zhi-Song, JIN Jie. Long-term outcome of isolated local recurrence following radical nephrectomy [J]. Journal of Peking University(Health Sciences), 2014, 46(4): 528-531. |
|
||