Journal of Peking University (Health Sciences) ›› 2026, Vol. 58 ›› Issue (3): 670-673. doi: 10.19723/j.issn.1671-167X.2026.03.030
Previous Articles Next Articles
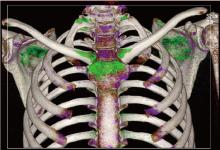
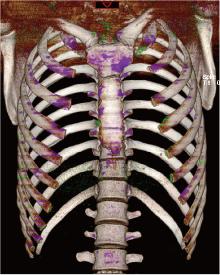
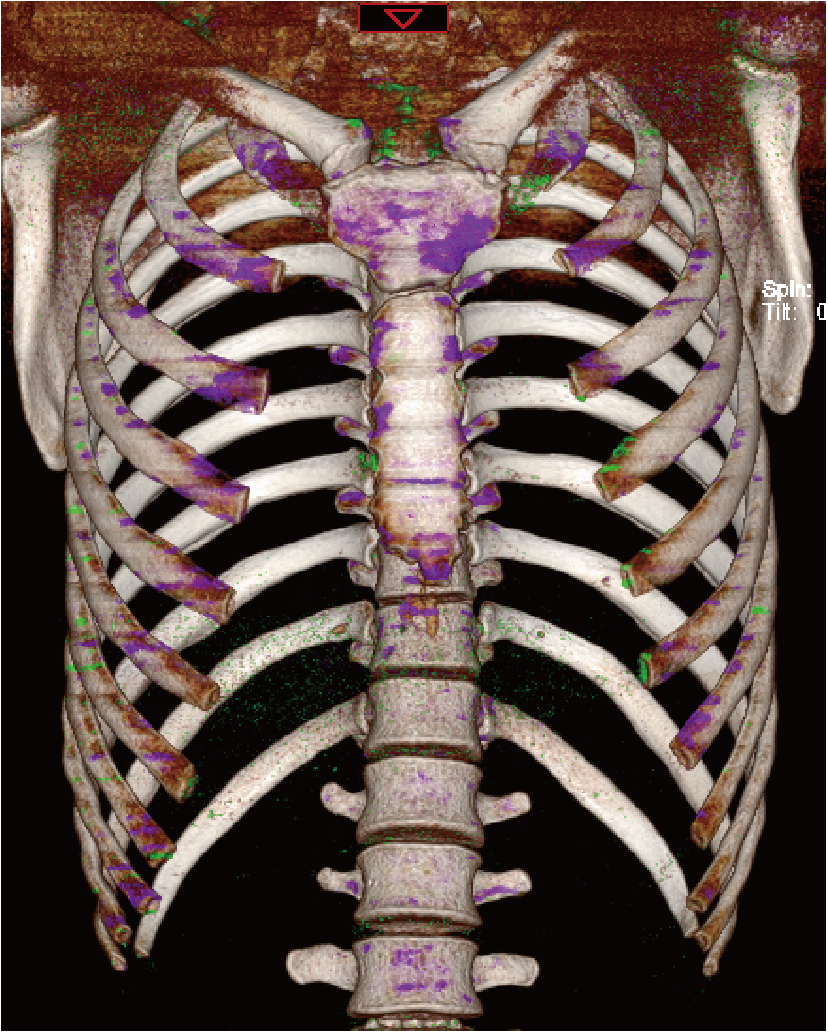
Gout of the manubriosternal joints: A case report
Di GAN1, Qiang FU1, Xiaohui TANG1, Chuwei LI1, Zhaoping SHU2,*( )
)
- 1. Department of Rheumatology and Immunology, The First Affiliated Hospital, Hengyang Medical School, University of South China, Hengyang 421001, Hunan, China
2. Department of Healthcare-associated Infection Management, The First Affiliated Hospital, Hengyang Medical School, University of South China, Hengyang 421001, Hunan, China
CLC Number:
- R589.7

| 1 |
doi: 10.1016/S0140-6736(21)00569-9 |
| 2 |
doi: 10.1136/annrheumdis-2015-208237 |
| 3 |
doi: 10.1136/annrheumdis-2019-215315 |
| 4 |
doi: 10.3899/jrheum.080938 |
| 5 |
doi: 10.1093/rheumatology/keaa923 |
| 6 |
doi: 10.1148/radiol.2015142631 |
| 7 |
|
| 8 |
doi: 10.1093/rheumatology/keab301 |
| 9 |
doi: 10.1164/rccm.201301-0097IM |
| 10 |
doi: 10.31486/toj.20.0143 |
| 11 |
doi: 10.4103/2156-7514.103058 |
| 12 |
doi: 10.1016/j.clinre.2011.09.003 |
| 13 |
|
| 14 |
doi: 10.1111/j.1524-4741.2011.01129.x |
| 15 |
中华医学会内分泌学分会. 中国高尿酸血症与痛风诊疗指南(2019)[J]. 中华内分泌代谢杂志, 2020, 36 (1): 1- 13.
|
| 16 |
doi: 10.1001/jama.2011.1169 |
| [1] | Wei LIU, Wen GUO, Zhe GUO, Chunyan LI, Yunlong LI, Siqi LIU, Liang ZHANG, Hui SONG. Risk factors associated with non-radiographic bone erosion in patients with gout [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 735-739. |
| [2] | Hong DONG,Li-min WANG,Zhi-qiang WANG,Yan-qing LIU,Xiao-gang ZHANG,Ming-ming ZHANG,Juan LIU,Zhen-bin LI. Diurnal differences in acute gout attacks: A clinical study of male gout patients [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 915-922. |
| [3] | Yi-lin YE,Heng LIU,Li-ping PAN,Wei-bing CHAI. Periprosthetic gout flare after total knee arthroplasty: A misdiagnostic case report [J]. Journal of Peking University (Health Sciences), 2023, 55(2): 362-365. |
| [4] | Yu WANG,Hui-min ZHANG,Xue-rong DENG,Wei-wei LIU,Lu CHEN,Ning ZHAO,Xiao-hui ZHANG,Zhi-bo SONG,Yan GENG,Lan-lan JI,Yu WANG,Zhuo-li ZHANG. Diagnostic values of urinary citrate for kidney stones in patients with primary gout [J]. Journal of Peking University (Health Sciences), 2022, 54(6): 1134-1140. |
| [5] | Xiao-wei XIE,Fen LI,Guang-hui LING,Xi XIE,Su-qing XU,Yi-yue CHEN. Development and clinical application of the health education knowledge assessment questionnaire for gout [J]. Journal of Peking University (Health Sciences), 2022, 54(4): 699-704. |
| [6] | PENG Zhe,DING Ya-min,PEI Lin,YAO Hai-hong,ZHANG Xue-wu,TANG Su-mei. Clinical characteristics of crystal deposits in joints and tendons in patients with gout [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1067-1071. |
| [7] | WANG Gui-hong,ZUO Ting,LI Ran,ZUO Zheng-cai. Effect of rebamipide on the acute gouty arthritis in rats induced by monosodium urate crystals [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 716-720. |
| [8] | XIE Yi-fan,WANG Yu,DENG Xue-rong,GENG Yan,JI Lan-lan,ZHANG Zhuo-li. Analysis of risk factors influencing the detection rate of urate crystal by dual energy computed tomography [J]. Journal of Peking University (Health Sciences), 2021, 53(2): 261-265. |
| [9] | WANG Yu,DENG Xue-rong,JI Lan-lan,ZHANG Xiao-hui,GENG Yan,ZHANG Zhuo-li. Risk factors and diagnostic value for ultrasound-detected tendon monosodium urate crystal deposition in patients with gout [J]. Journal of Peking University (Health Sciences), 2021, 53(1): 143-149. |
| [10] | Lan-lan JI,Yan-jie HAO,Zhuo-li ZHANG. A case of gout secondary to primary myelofibrosis [J]. Journal of Peking University(Health Sciences), 2018, 50(6): 1117-1119. |
| [11] | ZHANG Qian-ru, WANG Yu, ZHANG Zhuo-li. Performance of the 2015 ACR/EULAR classification criteria compared with other classification criteria for diagnosis of gout in Chinese patients [J]. Journal of Peking University(Health Sciences), 2017, 49(6): 979-984. |
|
||