Journal of Peking University (Health Sciences) ›› 2022, Vol. 54 ›› Issue (6): 1134-1140. doi: 10.19723/j.issn.1671-167X.2022.06.013
Previous Articles Next Articles
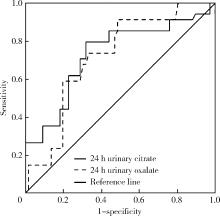
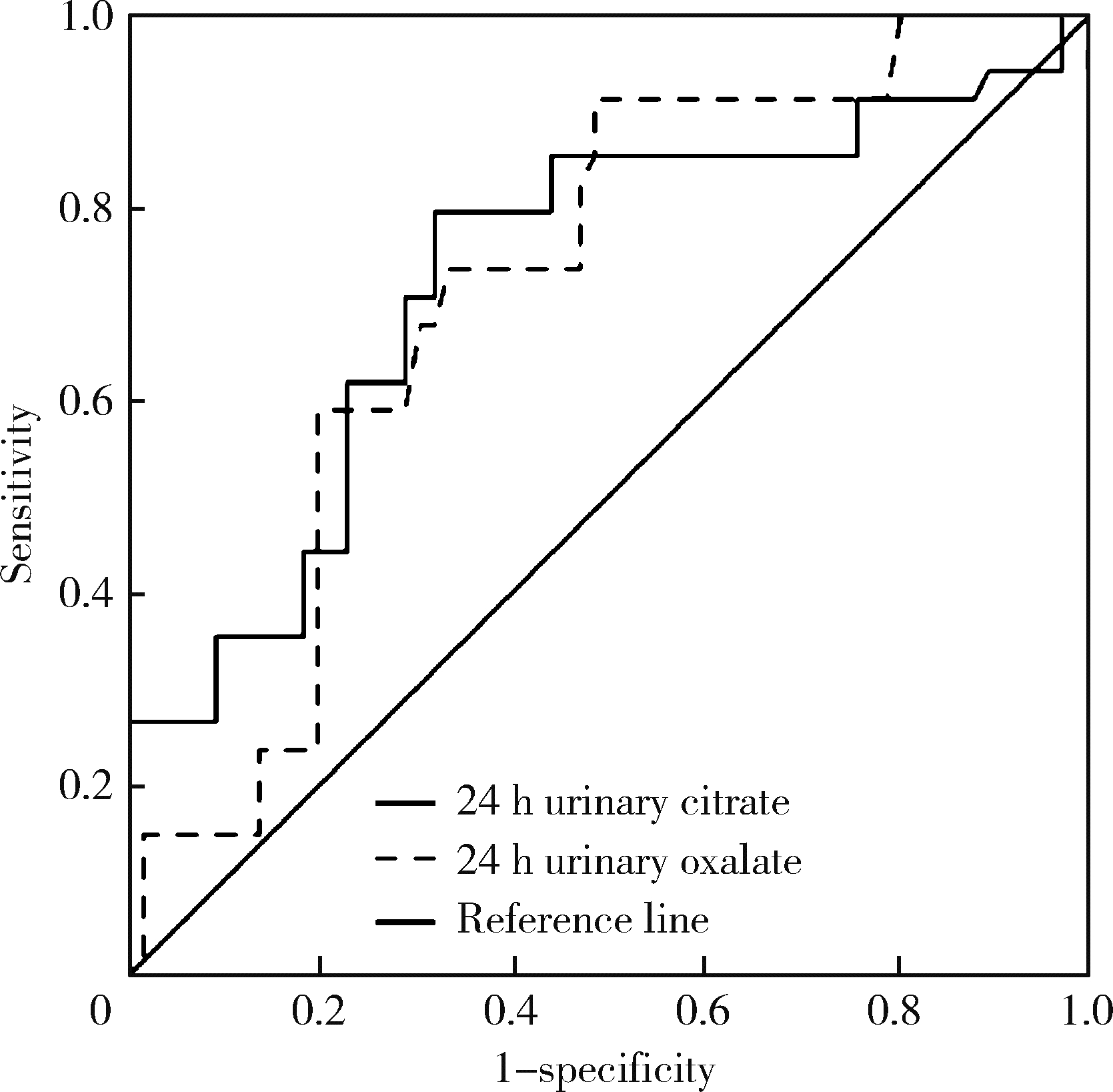
Diagnostic values of urinary citrate for kidney stones in patients with primary gout
Yu WANG1,Hui-min ZHANG2,Xue-rong DENG1,Wei-wei LIU3,Lu CHEN4,Ning ZHAO5,Xiao-hui ZHANG1,Zhi-bo SONG1,Yan GENG1,Lan-lan JI1,Yu WANG2,Zhuo-li ZHANG1,*( )
)
- 1. Department of Rheumatology and Immunology, Peking University First Hospital, Beijing 100034, China
2. Department of Nephrology, Peking University First Hospital, Beijing 100034, China
3. Department of Internal General Medicine, Zhongjie Hospital, Cangzhou 061108, Hebei, China
4. Department of Traditional Chinese Medicine, Aviation General Hospital of China Medical University, Beijing 100012, China
5. Department of Acupuncture, Huguosi Traditional Chinese Medicine Hospital affiliated to Beijing University of Chinese Medicine, Beijing 100035, China
CLC Number:
- R589.7
| 1 |
Wallace SL , Robinson H , Masi AT , et al. Preliminary criteria for the classification of the acute arthritis of primary gout[J]. Arthritis Rheum, 1977, 20 (3): 895- 900.
doi: 10.1002/art.1780200320 |
| 2 |
Filippou G , Pascart T , Iagnocco A . Utility of ultrasound and dual energy CT in crystal disease diagnosis and management[J]. Curr Rheumatol Rep, 2020, 22 (5): 15.
doi: 10.1007/s11926-020-0890-1 |
| 3 |
Skolarikos A , Straub M , Knoll T , et al. Metabolic evaluation and recurrence prevention for urinary stone patients: EAU guidelines[J]. Eur Urol, 2015, 67 (4): 750- 763.
doi: 10.1016/j.eururo.2014.10.029 |
| 4 |
Neogi T , Jansen TL , Dalbeth N , et al. 2015 gout classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative[J]. Ann Rheum Dis, 2015, 74 (10): 1789- 1798.
doi: 10.1136/annrheumdis-2015-208237 |
| 5 |
Gutierrez M , Schmidt WA , Thiele RG , et al. International consensus for ultrasound lesions in gout: Results of Delphi process and web-reliability exercise[J]. Rheumatology (Oxford), 2015, 54 (10): 1797- 1805.
doi: 10.1093/rheumatology/kev112 |
| 6 |
范兵, 王霄英, 邱建星, 等. 能谱CT与常规CT对泌尿系结石CT值的相关性分析[J]. CT理论与应用研究, 2016, 25 (4): 403- 408.
doi: 10.15953/j.1004-4140.2016.25.04.03 |
| 7 |
《泌尿外科杂志(电子版)》编辑部. 泌尿系结石诊治指南解读(一)[J]. 泌尿外科杂志(电子版), 2010, 2 (4): 56- 57.
doi: 10.3969/j.issn.1674-7410.2010.04.017 |
| 8 |
Richette P , Doherty M , Pascual E , et al. 2018 updated European League Against Rheumatism evidence-based recommendations for the diagnosis of gout[J]. Ann Rheum Dis, 2020, 79 (1): 31- 38.
doi: 10.1136/annrheumdis-2019-215315 |
| 9 |
王昱, 陈育青, 张蓓, 等. 原发性痛风患者24 h尿液化学成分分析与尿酸结石形成风险的研究[J]. 中华风湿病学杂志, 2018, 22 (3): 165- 170.
doi: 10.3760/cma.j.issn.1007-7480.2018.03.005 |
| 10 |
Tzelves L , Türk C , Skolarikos A . European Association of Urology urolithiasis guidelines: Where are we going?[J]. Eur Urol Focus, 2021, 7 (1): 34- 38.
doi: 10.1016/j.euf.2020.09.011 |
| 11 |
Pearle MS , Goldfarb DS , Assimos DG , et al. Medical management of kidney stones: AUA guideline[J]. J Urol, 2014, 192 (2): 316- 324.
doi: 10.1016/j.juro.2014.05.006 |
| 12 |
Nestler T , Nestler K , Neisius A , et al. Diagnostic accuracy of third-generation dual-source dual-energy CT: A prospective trial and protocol for clinical implementation[J]. World J Urol, 2019, 37 (4): 735- 741.
doi: 10.1007/s00345-018-2430-4 |
| 13 | 张晓洁, 姜林娣. 痛风患者肾脏结石与关节部位尿酸盐晶体沉积的相关性[J]. 中国临床医学, 2017, 24 (5): 767- 769. |
| 14 |
Siener R , Glatz S , Nicolay C , et al. Prospective study on the efficacy of a selective treatment and risk factors for relapse in recurrent calcium oxalate stone patients[J]. Eur Urol, 2003, 44 (4): 467- 474.
doi: 10.1016/S0302-2838(03)00317-8 |
| 15 |
Mittal A , Tandon S , Singla SK , et al. In vitro inhibition of cal-cium oxalate crystallization and crystal adherence to renal tubular epithelial cells by Terminalia arjuna[J]. Urolithiasis, 2016, 44 (2): 117- 125.
doi: 10.1007/s00240-015-0822-0 |
| 16 | 闫晓煜, 黄志红, 孟胜兰, 等. 24小时尿枸橼酸、草酸定量检测在泌尿系结石诊断中的应用[J]. 标记免疫分析与临床, 2018, 25 (5): 634- 668. |
| 17 |
Smith LH . Diet and hyperoxaluria in the syndrome of idiopathic calcium oxalate urolithiasis[J]. Am J Kidney Dis, 1991, 17 (4): 370- 375.
doi: 10.1016/S0272-6386(12)80625-1 |
| 18 |
Holmes RP , Goodman HO , Assimos DG . Contribution of dietary oxalate to urinary oxalate excretion[J]. Kidney Int, 2001, 59 (1): 270- 276.
doi: 10.1046/j.1523-1755.2001.00488.x |
| 19 |
Robijn S , Hoppe B , Vervaet BA , et al. Hyperoxaluria: A gut-kidney axis?[J]. Kidney Int, 2011, 80 (11): 1146- 1158.
doi: 10.1038/ki.2011.287 |
| 20 |
Taylor EN , Curhan GC . Oxalate intake and the risk for nephroli-thiasis[J]. J Am Soc Nephrol, 2007, 18 (7): 2198- 2204.
doi: 10.1681/ASN.2007020219 |
| 21 |
Curhan GC , Taylor EN . 24 h uric acid excretion and the risk of kidney stones[J]. Kidney Int, 2008, 73 (4): 489- 496.
doi: 10.1038/sj.ki.5002708 |
| 22 |
Kok DJ , Papapoulos SE , Bijvoet OL . Crystal agglomeration is a major element in calcium oxalate urinary stone formation[J]. Kidney Int, 1990, 37 (1): 51- 56.
doi: 10.1038/ki.1990.7 |
| 23 |
Mandel EI , Taylor EN , Curhan GC . Dietary and lifestyle factors and medical conditions associated with urinary citrate excretion[J]. Clin J Am Soc Nephrol, 2013, 8 (6): 901- 908.
doi: 10.2215/CJN.07190712 |
| 24 |
Domrongkitchaiporn S , Stitchantrakul W , Kochakarn W . Causes of hypocitraturia in recurrent calcium stone formers: Focusing on urinary potassium excretion[J]. Am J Kidney Dis, 2006, 48 (4): 546- 554.
doi: 10.1053/j.ajkd.2006.06.008 |
| 25 |
Coe FL , Parks JH , Asplin JR . The pathogenesis and treatment of kidney stones[J]. N Engl J Med, 1992, 327 (16): 1141- 1152.
doi: 10.1056/NEJM199210153271607 |
| 26 |
Ettinger B , Tang A , Citron JT , et al. Randomized trial of allopurinol in the prevention of calcium oxalate calculi[J]. N Engl J Med, 1986, 315 (22): 1386- 1389.
doi: 10.1056/NEJM198611273152204 |
| 27 |
Ferraro PM , Curhan GC , D'Addessi A , et al. Risk of recurrence of idiopathic calcium kidney stones: Analysis of data from the lite-rature[J]. J Nephrol, 2017, 30 (2): 227- 233.
doi: 10.1007/s40620-016-0283-8 |
| 28 |
Levy FL , Adams-Huet B , Pak CY . Ambulatory evaluation of nephrolithiasis: An update of a 1980 protocol[J]. Am J Med, 1995, 98 (1): 50- 59.
doi: 10.1016/S0002-9343(99)80080-1 |
| [1] | Jinfang YUAN, Xinli WANG, Yunpu CUI, Xuemei WANG. Application of urinary luteinizing hormone in the prediction of central precocious puberty in girls [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 788-793. |
| [2] | Yan CHEN,Kuangmeng LI,Kai HONG,Shudong ZHANG,Jianxing CHENG,Zhongjie ZHENG,Wenhao TANG,Lianming ZHAO,Haitao ZHANG,Hui JIANG,Haocheng LIN. Retrospective study on the impact of penile corpus cavernosum injection test on penile vascular function [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 680-686. |
| [3] | Yue WEI,Lan YAO,Xi LU,Jun WANG,Li LIN,Kun-peng LIU. Evaluation of gastric emptying after drinking carbohydrates before cesarean section by gastric ultrasonography [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1082-1087. |
| [4] | Yue WEI,Xi LU,Jing ZHANG,Kun-peng LIU,Yong-jun WANG,Lan YAO. Effect of preoperative carbohydrates intake on the gastric volume and the risk of reflux aspiration in patients positioning in trendelenburg undergoing gynecological laparoscopic procedures [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 893-898. |
| [5] | Hong DONG,Li-min WANG,Zhi-qiang WANG,Yan-qing LIU,Xiao-gang ZHANG,Ming-ming ZHANG,Juan LIU,Zhen-bin LI. Diurnal differences in acute gout attacks: A clinical study of male gout patients [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 915-922. |
| [6] | Qiang FU,Guan-ying GAO,Yan XU,Zhuo-hua LIN,You-jing SUN,Li-gang CUI. Comparative study of ultrasound and magnetic resonance imaging in the diagnosis of asymptomatic anterosuperior acetabular labrum tears [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 665-669. |
| [7] | Yi-lin YE,Heng LIU,Li-ping PAN,Wei-bing CHAI. Periprosthetic gout flare after total knee arthroplasty: A misdiagnostic case report [J]. Journal of Peking University (Health Sciences), 2023, 55(2): 362-365. |
| [8] | Hai-ying XING,Yu-hui CHEN,Ke XU,Dian-dian HUANG,Qing PENG,Ran LIU,Wei SUN,Yi-ning HUANG. Evaluation of carotid atherosclerotic plaques by vascular plaque quantification (VPQ) technology of three-dimensional ultrasonography [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 991-999. |
| [9] | Xiao-wei XIE,Fen LI,Guang-hui LING,Xi XIE,Su-qing XU,Yi-yue CHEN. Development and clinical application of the health education knowledge assessment questionnaire for gout [J]. Journal of Peking University (Health Sciences), 2022, 54(4): 699-704. |
| [10] | PENG Zhe,DING Ya-min,PEI Lin,YAO Hai-hong,ZHANG Xue-wu,TANG Su-mei. Clinical characteristics of crystal deposits in joints and tendons in patients with gout [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1067-1071. |
| [11] | WANG Gui-hong,ZUO Ting,LI Ran,ZUO Zheng-cai. Effect of rebamipide on the acute gouty arthritis in rats induced by monosodium urate crystals [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 716-720. |
| [12] | XIE Yi-fan,WANG Yu,DENG Xue-rong,GENG Yan,JI Lan-lan,ZHANG Zhuo-li. Analysis of risk factors influencing the detection rate of urate crystal by dual energy computed tomography [J]. Journal of Peking University (Health Sciences), 2021, 53(2): 261-265. |
| [13] | YANG Guang-xin,LUAN Jing-yuan,JIA Zi-chang. Radiofrequency obliteration of varicose veins of lower extremity guided by combined venography and ultrasonography [J]. Journal of Peking University (Health Sciences), 2021, 53(2): 332-336. |
| [14] | WANG Yu,DENG Xue-rong,JI Lan-lan,ZHANG Xiao-hui,GENG Yan,ZHANG Zhuo-li. Risk factors and diagnostic value for ultrasound-detected tendon monosodium urate crystal deposition in patients with gout [J]. Journal of Peking University (Health Sciences), 2021, 53(1): 143-149. |
| [15] | Ming-rui WANG,Qi WANG,Hao HU,Jin-hui LAI,Yong-xin HE,Jie XIONG,Xian-hui LIU,Shi-jun LIU,Ke-xin XU,Tao XU. Long-term analysis of safety and efficacy of standard percutaneous nephrolithotomy in patients with solitary kidneys [J]. Journal of Peking University (Health Sciences), 2020, 52(4): 663-666. |
|
||