Journal of Peking University (Health Sciences) ›› 2020, Vol. 52 ›› Issue (3): 500-505. doi: 10.19723/j.issn.1671-167X.2020.03.016
Previous Articles Next Articles
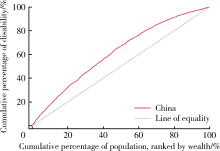
Research on equity and influencing factors of disability among Chinese middle-aged and old people
Zhe-bin WANG,Zhi-jie ZHENG( )
)
- Department of Global Health, Peking University School of Public Health, Beijing 100191, China
CLC Number:
- R197.1

| [1] | World Health Organization. World report on ageing and health [R]. Geneva: World Health Organization, 2015: 246. |
| [2] | Jones GW. Ageing in China, India and Indonesia: an overview[M] // Contemporary demographic transformations in China, India and Indonesia. Berlin: Springer, 2016: 325-328. |
| [3] | United Nations. Department of economic and social affairs, population division (2013), world population ageing 2013[M]. New York: United Nations publication, 2013. |
| [4] |
Crimmins EM, Beltrán-Sánchez H. Mortality and morbidity trends: is there compression of morbidity?[J]. J Gerontol B Psychol Sci Soc Sci, 2011,66(1):75-86.
pmid: 21135070 |
| [5] | Wang XQ, Chen PJ. Population ageing challenges health care in China[J]. Lancet, 2014,383(9920):870. |
| [6] | Du P, Wang Y. Population ageing and the development of social care service systems for older persons in China[J]. Int J Ageing Dev C, 2016,1(1):40-52. |
| [7] | Chen X, Huang B, Li S. Population ageing and inequality: Evidence from China[J]. World Economy, 2018,41(8):1976-2000. |
| [8] | Fan C, Ouyang W, Tian L, et al. Elderly health inequality in China and its determinants: a geographical perspective[J]. Int J Environ Res Public Health, 2019,16(16):2953. |
| [9] | Zhong Y, Wang J, Nicholas S. Gender, childhood and adult socioeconomic inequalities in functional disability among Chinese older adults[J]. Int J Equity Health, 2017,16(1):165. |
| [10] |
Yang L, Konttinen H, Martikainen P, et al. Socioeconomic status and physical functioning: a longitudinal study of older Chinese people[J]. J Gerontol B Psychol Sci Soc Sci, 2018,73(7):1315-1329.
pmid: 28329825 |
| [11] | International Health Conference. Constitution of the World Health Organization. 1946[J]. Bull World Health Organ, 2002,80(12):983-984. |
| [12] | O’Donnell O, Doorslaer EV, Wagstaff A, et al. Analyzing health equity using household survey data: A guide to techniques and their implementation[J]. World Bank, 2008,86(10):816-816. |
| [13] | Üstuün TB, Ebrary I. Measuring health and disability: manual for WHO Disability Assessment Schedule WHODAS 2.0 [R]. Geneva: World Health Organization, 2010. |
| [14] | Murray CJL, Evans DB. Health systems performance assessment: Debates, methods and empiricism[M]. Geneva: World Health Organization, 2003. |
| [15] |
Bull FC, Maslin TS, Armstrong T. Global physical activity questionnaire (GPAQ): nine country reliability and validity study[J]. J Phys Act Health, 2009,6(6):790-804.
doi: 10.1123/jpah.6.6.790 pmid: 20101923 |
| [16] | Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ)[J]. J Public Health, 2006,14(2):66-70. |
| [17] |
van Doorslaer E, Koolman X. Explaining the differences in income—related health inequalities across European countries[J]. Health Econ, 2004,13(7):609-628.
pmid: 15259042 |
| [18] | Macinko J, Harris MJ, Rocha MG. Brazil’s National Program for Improving Primary Care Access and Quality (PMAQ): fulfilling the potential of the world’s largest payment for performance system in primary care[J]. J Ambul Care Manage, 2017,40(2 Suppl):S4-S11. |
| [19] | 赵梓行. 均等化视角下印度医疗服务体系管理研究[D]. 湖南: 湘潭大学, 2018. |
| [20] | Adriano M, Thomas H, Gomes LFA, et al. The Brazilian health system at crossroads: progress, crisis and resilience[J]. BMJ Global Health, 2018,3(4):e000829. |
| [21] |
Balarajan Y, Selvaraj S, Subramanian SV. Health care and equity in India[J]. Lancet, 2011,377(9764):505-515.
pmid: 21227492 |
| [22] | Sharma JK, Narang R. Quality of healthcare services in rural India: the user perspective[J]. Vikalpa, 2011,36(1):51-60. |
| [1] | Abudurexiti ANARGUL, Yinghao SONG, Xiaojin YAN, Yongkang GAO, Bo LIU, Gang HU. Disease burden and future trend predictions of age-related hearing loss in China and worldwide from 1990 to 2021 [J]. Journal of Peking University (Health Sciences), 2025, 57(3): 545-553. |
| [2] | Haoyu ZHANG,Yiwen SHI,Wei PAN,Aiping LIU,Xinying SUN,Man LI,Xuxi ZHANG. Factors associated with the care needs of the older adults based on different disability levels [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 431-440. |
| [3] | Xiaohan LIU,Fan YANG,Xindi WANG,Ning HUANG,Taozhu CHENG,Jing GUO. Related factors and equity of health status among floating population in China based on geographic information system analysis [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 223-229. |
| [4] | ZHANG Lei, ZHU Lei, LI Zhi-Heng, LI Jin-Zhou, PAN Hong-Wei, ZHANG Shao-Feng, QIN Wen-Hua, HE Li-Hua. Analysis on the disease burden and its impact factors of coal worker’s pneumoconiosis inpatients [J]. Journal of Peking University(Health Sciences), 2014, 46(2): 226-231. |
|
||