Journal of Peking University (Health Sciences) ›› 2022, Vol. 54 ›› Issue (4): 692-698. doi: 10.19723/j.issn.1671-167X.2022.04.018
Previous Articles Next Articles
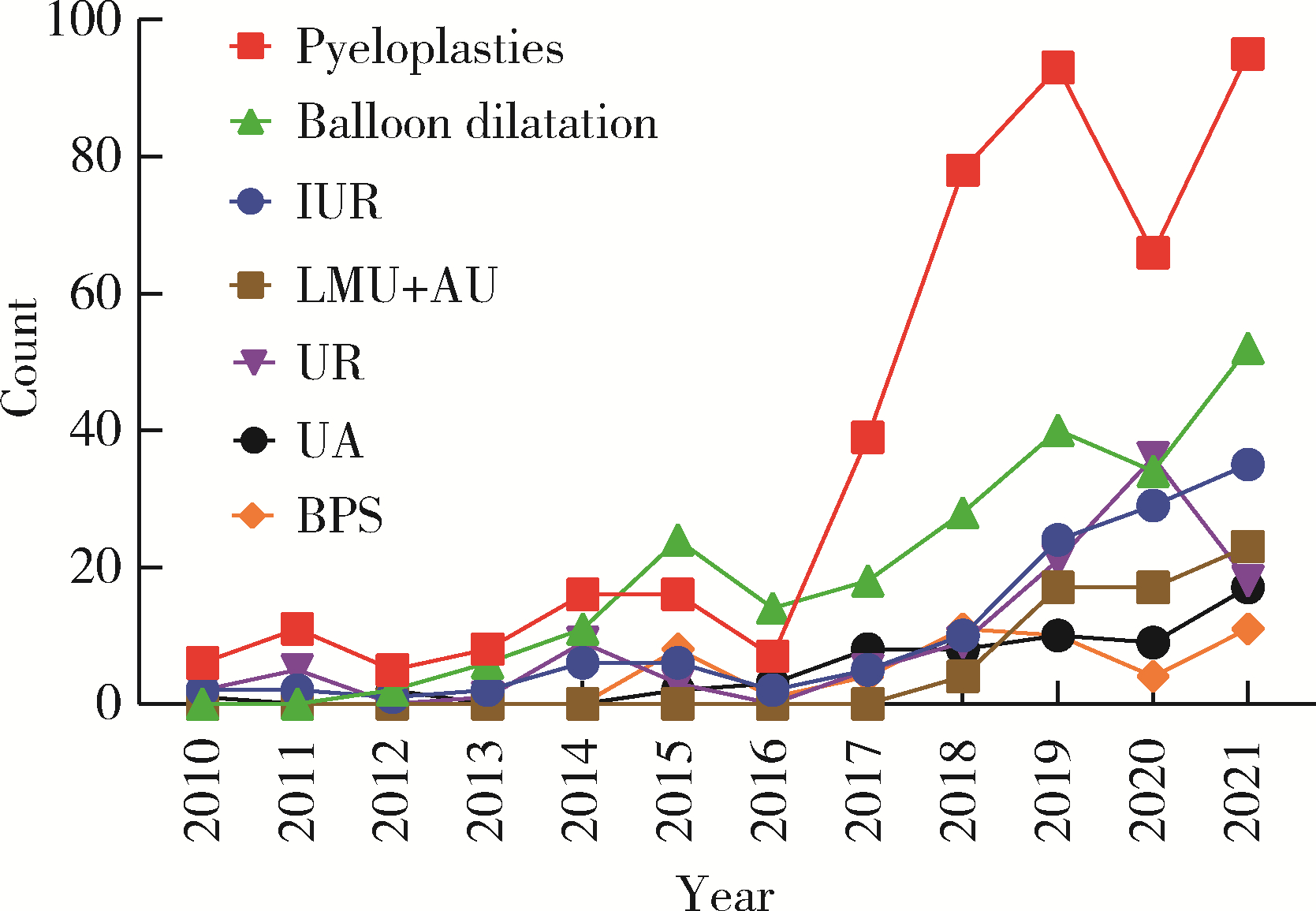
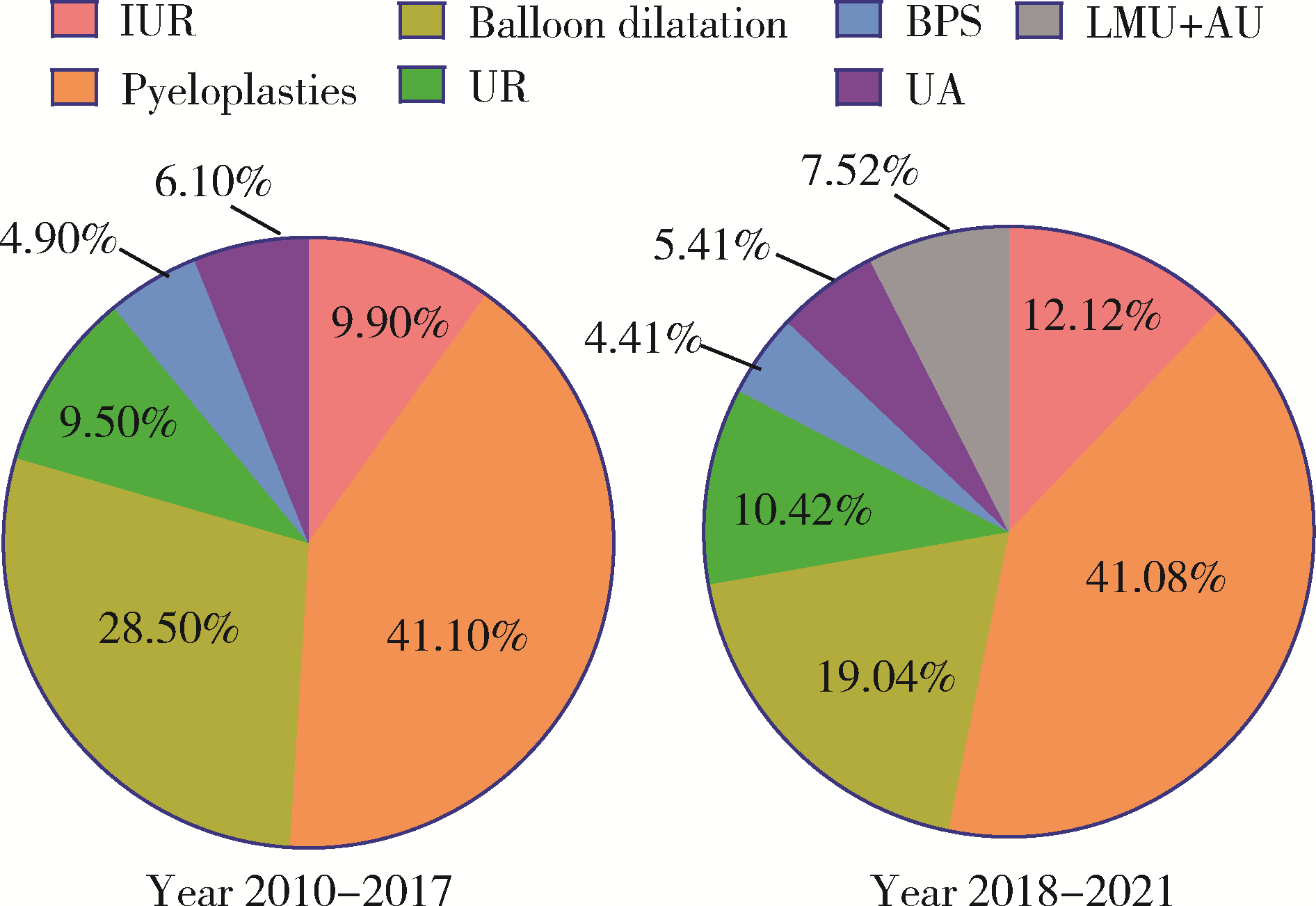
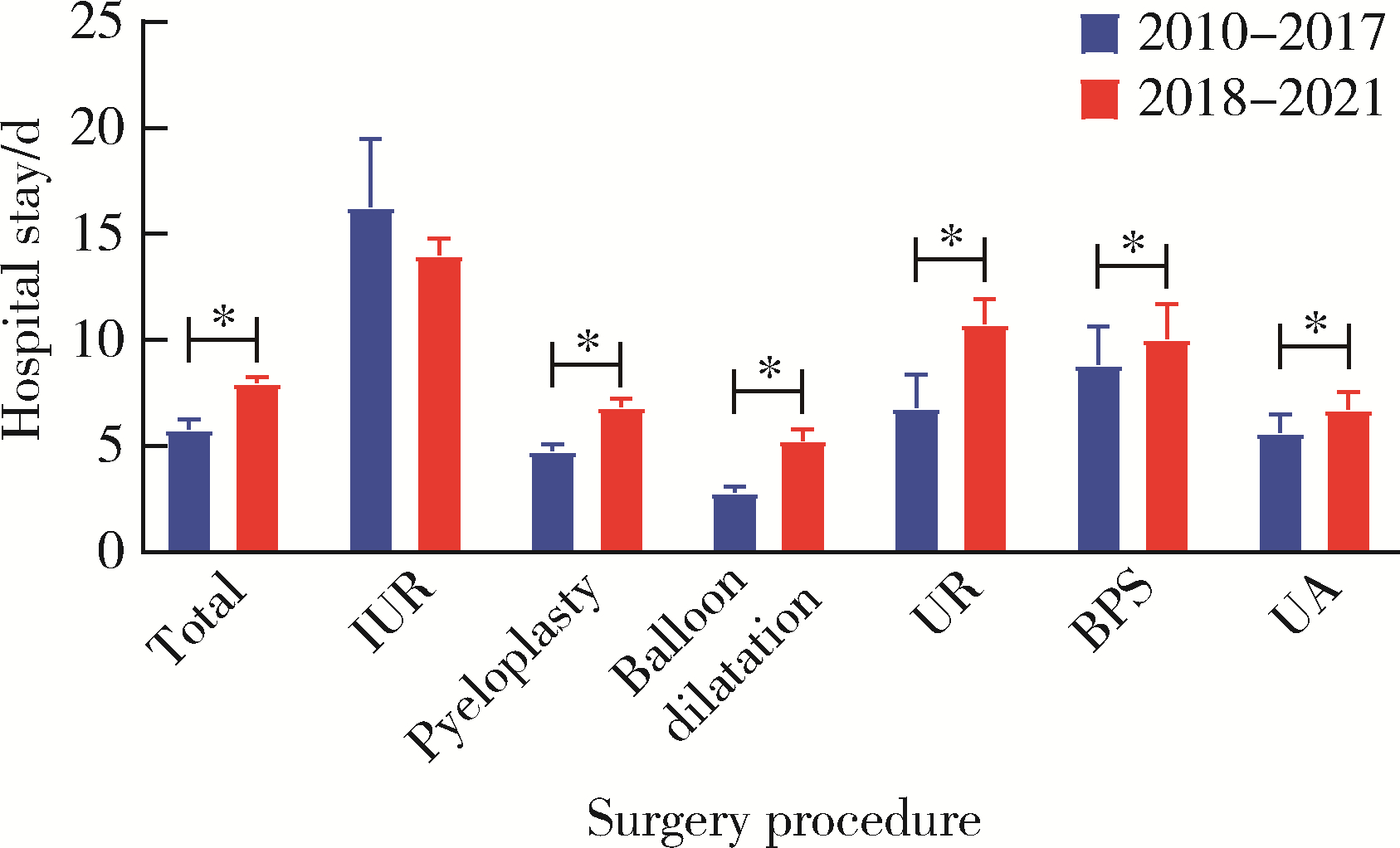
Trends in upper urinary tract reconstruction surgery over a decade based on a multi-center database
Wei ZUO1,Fei GAO1,Chang-wei YUAN1,Sheng-wei XIONG1,Zhi-hua LI1,Lei ZHANG1,Kun-lin YANG1,Xin-fei LI1,Liang LIU2,Lai WEI2,Peng ZHANG3,Bing WANG4,Ya-ming GU4,Hong-jian ZHU2,Zheng ZHAO1,*( ),Xue-song LI1,*()
),Xue-song LI1,*()
- 1. Department of Urology, Peking University First Hospital; Institute of Urology, Peking University; National Urological Cancer Center, Beijing 100034, China
2. Department of Urology, Beijing Jiangong Hospital, Beijing 100054, China
3. Department of Urology, Emergency General Hospital, Beijing 100028, China
4. Department of Urology, Miyun District Hospital (Miyun Hospital, Peking University First Hospital), Beijing 101599, China
CLC Number:
- R691.6





| 1 |
Stief CG , Jonas U , Petry KU , et al. Ureteric reconstruction[J]. BJU international, 2003, 91 (2): 138- 142.
doi: 10.1046/j.1464-410X.2003.03060.x |
| 2 |
Zhu W , Xiong S , Xu C , et al. Initial experiences with preoperative three-dimensional image reconstruction technology in laparoscopic pyeloplasty for ureteropelvic junction obstruction[J]. Transl Androl Urol, 2021, 10 (11): 4142- 4151.
doi: 10.21037/tau-21-590 |
| 3 |
Yuan C , Wang J , Cheng S , et al. Robotic ureteral reimplantation for the management of ureterovaginal fistula: Four cases at a single center[J]. Transl Androl Urol, 2021, 10 (10): 3705- 3713.
doi: 10.21037/tau-21-454 |
| 4 |
Yang K , Fan S , Wang J , et al. Robotic-assisted lingual mucosal graft ureteroplasty for the repair of complex ureteral strictures: Technique description and the medium-term outcome[J]. Eur Urol, 2022, 81 (5): 533- 540.
doi: 10.1016/j.eururo.2022.01.007 |
| 5 |
Wang J , Xiong S , Fan S , et al. Appendiceal onlay flap ureteroplasty for the treatment of complex ureteral strictures: Initial experience of nine patients[J]. J Endourol, 2020, 34 (8): 874- 881.
doi: 10.1089/end.2020.0176 |
| 6 |
Fan S , Yin L , Yang K , et al. Posteriorly augmented anastomotic ureteroplasty with lingual mucosal onlay grafts for long proximal ureteral strictures: 10 cases of experience[J]. J Endourol, 2021, 35 (2): 192- 199.
doi: 10.1089/end.2020.0686 |
| 7 |
Li X , Wang X , Li T , et al. Cine magnetic resonance urography and whitaker test: Dynamic visualized and quantified tools in ileal ureter replacement[J]. Transl Androl Urol, 2021, 10 (11): 4110- 4119.
doi: 10.21037/tau-21-507 |
| 8 | Li X , Yang K , Zhu W , et al. The whitaker test in the follow-up of complex upper urinary tract reconstruction: Is it clinical useful or not[J]. Urol J, 2021, 19 (1): 56- 62. |
| 9 | Ding G , Li X , Fang D , et al. Etiology and ureteral reconstruction strategy for iatrogenic ureteral injuries: A retrospective single-center experience[J]. Urol Int, 2021, 105 (5/6): 470- 476. |
| 10 |
de Onis M , Blössner M . The world health organization global database on child growth and malnutrition: Methodology and applications[J]. Int J Epidemiol, 2003, 32 (4): 518- 526.
doi: 10.1093/ije/dyg099 |
| 11 |
Jacobs JP , Lacour-Gayet FG , Jacobs ML , et al. Initial application in the sts congenital database of complexity adjustment to evaluate surgical case mix and results[J]. Ann Thorac Surg, 2005, 79 (5): 1635- 1649.
doi: 10.1016/j.athoracsur.2004.09.065 |
| 12 |
Kakeji Y , Yamamoto H , Ueno H , et al. Development of gastroenterological surgery over the last decade in japan: Analysis of the national clinical database[J]. Surg Today, 2021, 51 (2): 187- 193.
doi: 10.1007/s00595-020-02075-7 |
| 13 |
Bowdish ME , D'Agostino RS , Thourani VH , et al. Sts adult car-diac surgery database: 2021 update on outcomes, quality, and research[J]. Ann Thorac Surg, 2021, 111 (6): 1770- 1780.
doi: 10.1016/j.athoracsur.2021.03.043 |
| 14 |
Kwoh YS , Hou J , Jonckheere EA , et al. A robot with improved absolute positioning accuracy for ct guided stereotactic brain surgery[J]. IEEE Trans Biomed Eng, 1988, 35 (2): 153- 160.
doi: 10.1109/10.1354 |
| 15 |
Binder J , Kramer W . Robotically-assisted laparoscopic radical prostatectomy[J]. BJU Int, 2001, 87 (4): 408- 410.
doi: 10.1046/j.1464-410x.2001.00115.x |
| 16 |
Rosero EB , Kho KA , Joshi GP , et al. Comparison of robotic and laparoscopic hysterectomy for benign gynecologic disease[J]. Obstet Gynecol, 2013, 122 (4): 778- 786.
doi: 10.1097/AOG.0b013e3182a4ee4d |
| 17 |
Yates DR , Vaessen C , Roupret M . From leonardo to da vinci: The history of robot-assisted surgery in urology[J]. BJU Int, 2011, 108 (11): 1708- 1713.
doi: 10.1111/j.1464-410X.2011.10576.x |
| 18 |
Autorino R , Porpiglia F , Dasgupta P , et al. Precision surgery and genitourinary cancers[J]. Eur J Surg Oncol, 2017, 43 (5): 893- 908.
doi: 10.1016/j.ejso.2017.02.005 |
| 19 |
Leal Ghezzi T , Campos Corleta O . 30 years of robotic surgery[J]. World J Surg, 2016, 40 (10): 2550- 2557.
doi: 10.1007/s00268-016-3543-9 |
| 20 |
Andolfi C , Adamic B , Oommen J , et al. Robot-assisted laparoscopic pyeloplasty in infants and children: Is it superior to conventional laparoscopy?[J]. World J Urol, 2020, 38 (8): 1827- 1833.
doi: 10.1007/s00345-019-02943-z |
| 21 |
Crocerossa F , Carbonara U , Cantiello F , et al. Robot-assisted radical nephrectomy: A systematic review and meta-analysis of comparative studies[J]. Eur Urol, 2021, 80 (4): 428- 439.
doi: 10.1016/j.eururo.2020.10.034 |
| 22 |
Deng T , Liu B , Luo L , et al. Robot-assisted laparoscopic versus open ureteral reimplantation for pediatric vesicoureteral reflux: A systematic review and meta-analysis[J]. World J Urol, 2018, 36 (5): 819- 828.
doi: 10.1007/s00345-018-2194-x |
| [1] | Jiale GAO, Zhongtao ZHANG. Current status and future perspectives of precision treatment for locally advanced rectal cancer [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 247-250. |
| [2] | Bin LI, Han LIANG. Robotic gastrectomy: Research progress and practical challenges [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 416-422. |
| [3] | Lu YU, Ling WU, Xiaojing LIU, Zili LI. Feasibility study of a surgical planning protocol for orthognathic surgery utilizing similarity retrieval from database: A randomized controlled trial [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 145-152. |
| [4] | Shenmo LI, Dandan SU, Jiyu LIN, Haodong SONG, Lulin MA, Xiaofei HOU, Guoliang WANG, Hongxian ZHANG, Jianfei YE, Shudong ZHANG. Prognostic analysis of laparoscopic simultaneous radical cystectomy and nephroureterectomy [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 961-966. |
| [5] | Zonghan LI, Yangyue HUANG, Ning LI, Minglei LI, Hongcheng SONG, Weiping ZHANG, Chao LIU. Preliminary application of domestic single-port serpentine arm robotic surgical system in children's pyeloplasty [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 662-665. |
| [6] | Qiming ZHANG, Zebo CHEN, Yu TIAN, Dameng PAN, Lei LIU, Hongxian ZHANG, Lei ZHAO, Shudong ZHANG, Lulin MA, Xiaofei HOU. Experience summary of robot-assisted laparoscopic transplant nephrectomy [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 666-669. |
| [7] | Shihao LIU, Liqing XU, Xinfei LI, Kunlin YANG, Zhaoying LI, Zibo ZHANG, Xiang WANG, Wei-xiao FU, Zhihua LI, Xuesong LI. Evaluation of the feasibility and safety of a Chinese developed modular surgical robotic system for robot-assisted pyeloplasty [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 779-783. |
| [8] | Huanrui WANG, Shicong LAI, Haopu HU, Zehua DING, Tao XU, Hao HU. Efficacy analysis of laparoscopy combined with flexible ureteroscope in the treatment of complex ureteral stricture [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 784-788. |
| [9] | Shuai LIU, Zhuo LIU, Yunhe GUAN, Guoliang WANG, Xiaojun TIAN, Hongxian ZHANG, Lei LIU, Lulin MA, Shudong ZHANG. Robot-assisted laparoscopic inferior vena cava segmental resection for renal tumor with tumor thrombus invading the vascular wall [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 796-802. |
| [10] | Shiyu QIU, Yang LIAN, Yifan KANG, Lei ZHANG, Yiwang CAI, Xiaofeng SHAN, Zhigang CAI. Personalized mandibular reconstruction assisted by three-dimensional retrieval model based on fully connected neural network and a database of mandibles [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 360-368. |
| [11] | Silu CHEN, Haiju WANG, Yucai WU, Zhihua LI, Yanbo HUANG, Yuhui HE, Yangyang XU, Xuesong LI, Hua GUAN. Etiological analysis of hydronephrosis in adults: A single-center cross-sectional study [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 913-918. |
| [12] | Yicen YING,Yicong DU,Zhihua LI,Yiming ZHANG,Xinfei LI,Bing WANG,Peng ZHANG,Hongjian ZHU,Liqun ZHOU,Kunlin YANG,Xuesong LI. Robot-assisted laparoscopic ureteroplasty with buccal mucosa graft for complex ureteral stricture [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 640-645. |
| [13] | Jian-xun MA,You-chen XIA,Bi LI,Hong-mei ZHAO,Yu-tao LEI,Xi BU. Choice of immediate breast reconstructive methods after modified radical mastectomy [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 612-618. |
| [14] | LAN Lin,HE Yang,AN Jin-gang,ZHANG Yi. Relationship between prognosis and different surgical treatments of zygomatic defects: A retrospective study [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 356-362. |
| [15] | DING Ting-ting,ZENG Chu-xiong,HU Li-na,YU Ming-hua. Establishment of a prediction model for colorectal cancer immune cell infiltration based on the cancer genome atlas (TCGA) database [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 203-208. |
|
||