北京大学学报(医学版) ›› 2018, Vol. 50 ›› Issue (6): 1049-1052. doi: 10.19723/j.issn.1671-167X.2018.06.019
人工韧带在耻骨肿瘤切除后重建下腹壁缺损中的应用
臧杰,郭卫( ),汤小东,曲华毅,李大森
),汤小东,曲华毅,李大森
- 北京大学人民医院骨与软组织肿瘤治疗中心, 北京 100044
Application of artificial ligament in treatment of lower abdominal wall reconstruction after pubic tumor resection
Jie ZANG,Wei GUO(),Xiao-dong TANG,Hua-yi QU,Da-sen LI
- Musculoskeletal Tumor Center, Peking University People’s Hospital, Beijing 100044, China
摘要:
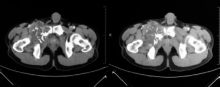
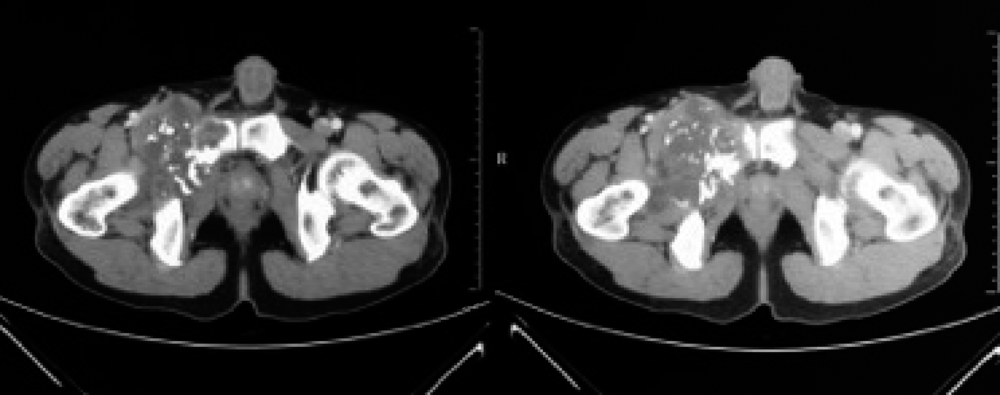
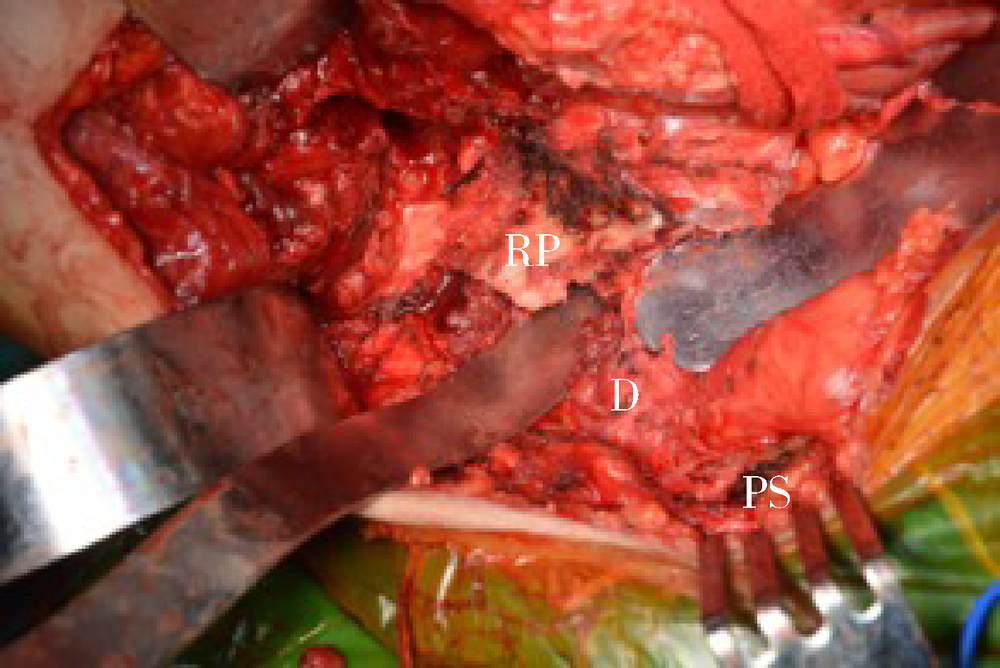
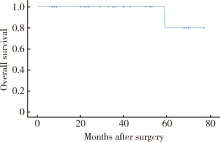
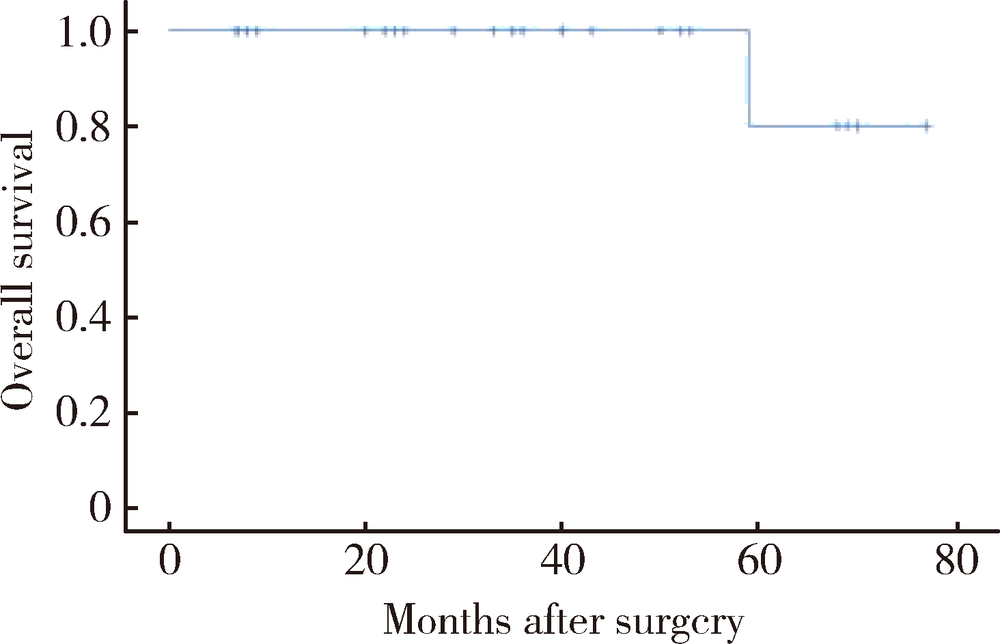
目的: 从患者的主观角度和临床客观指标评价人工韧带用于耻骨肿瘤切除后重建的临床效果。方法: 选择2012年2月至2018年2月因耻骨肿瘤就诊于北京大学人民医院骨与软组织肿瘤治疗中心,并接受手术切除和人工韧带重建的25例患者进行回顾性分析,评价其临床疗效以及相关并发症。结果: 所有患者均顺利接受手术,单纯切除耻骨上支的患者8例,耻骨下支5例,耻骨上下支一并切除的12例。平均出血量(774±580) mL,平均手术时间(138±25) min,平均住院时间(19±6) d。1例患者术后出现伤口愈合问题,经清创后愈合。平均随访时间为(37±21)个月,肿瘤复发1例,1例转移癌(肾癌)患者因原发肿瘤进展而死亡。无切口疝,无韧带感染以及局部异物感等相关并发症。23例患者术后活动不需要借助任何辅助设施,2例患者活动时需要拄单拐。19例患者未诉任何疼痛不适,3例患者诉活动时感轻度疼痛,3例患者中度疼痛。评价术后功能的MSTS评分平均为87±4。结论: 人工韧带可应用于耻骨肿瘤切除后下腹壁缺损的重建,此重建方式可以预防腹壁疝的发生,同时可以通过减小残腔而降低术后感染的发生率,从而获得患者术后较好的主观评价。
中图分类号:
- R738.1







| [1] |
Enneking WF, Dunham WK . Resection and reconstruction for primary neoplasms involving the innominate bone[J]. J Bone Joint Surg Am, 1978,60(6):731-746.
doi: 10.2106/00004623-197860060-00002 pmid: 701308 |
| [2] |
Angelini A, Drago G, Trovarelli G , et al. Infection after surgical resection for pelvic bone tumors: an analysis of 270 patients from one institution[J]. Clin Orthop Relat Res, 2014,472(1):349-359.
doi: 10.1007/s11999-013-3250-x pmid: 3889428 |
| [3] |
Karim SM, Colman MW, Lozano-Calderon SA , et al. What are the functional results and complications from allograft reconstruction after partial hemipelvectomy of the pubis[J]. Clin Orthop Relat Res, 2015,473(4):1442-1448.
doi: 10.1007/s11999-014-4009-8 pmid: 4353538 |
| [4] |
Mankin HJ, Hornicek FJ . Internal hemipelvectomy for the management of pelvic sarcomas[J]. Surg Oncol Clin N Am, 2005,14(2):381-396.
doi: 10.1016/j.soc.2004.11.010 pmid: 15817245 |
| [5] |
Die Trill J, Madrid JM, Ferrero E , et al. Posthemipelvectomy hernia[J]. Hernia, 2005,9(4):375-377.
doi: 10.1007/s10029-005-0328-8 pmid: 15912261 |
| [6] |
Reddy SS, Bloom ND . En bloc resection of extra-peritoneal soft tissue neoplasms incorporating a type Ⅲ internal hemipelvectomy: a novel approach[J]. World J Surg Oncol, 2012,10:222.
doi: 10.1186/1477-7819-10-222 pmid: 3543210 |
| [7] |
Sternberg A, Yosipovich Z . Primary marlex-mesh reconstruction in partial resections of the hemipelvis. Report of 2 cases[J]. Acta Orthop Scand, 1989,60(3):365-368.
doi: 10.3109/17453678909149296 pmid: 2750517 |
| [8] |
Chao AH, Neimanis SA, Chang DW , et al. Reconstruction after internal hemipelvectomy: outcomes and reconstructive algorithm[J]. Ann Plast Surg, 2015,74(3):342-349.
doi: 10.1097/SAP.0b013e31829778e1 |
| [9] |
Lavoie P, Fletcher J, Duval N . Patient satisfaction needs as related to knee stability and objective findings after ACL reconstruction using the LARS artificial ligament[J]. Knee, 2000,7(3):157-163.
doi: 10.1016/S0968-0160(00)00039-9 pmid: 10927209 |
| [10] |
Parchi PD, Ciapini G, Paglialunga C , et al. Anterior cruciate ligament reconstruction with LARS artificial ligament-clinical results after a long-term follow-up[J]. Joints, 2018,6(2):75-79.
doi: 10.1055/s-0038-1653950 |
| [11] |
Wang XM, Ji G, Wang XM , et al. Biological and biomechanical evaluation of autologous tendon combined with ligament advanced reinforcement system artificial ligament in a rabbit model of anterior cruciate ligament reconstruction[J]. Orthop Surg, 2018,10(2):144-151.
doi: 10.1111/os.12370 pmid: 29624874 |
| [12] |
Wilson RJ, Freeman TH Jr, Halpern JL , et al. Surgical outcomes after limb-sparing resection and reconstruction for pelvic sarcoma: asystematic review[J]. JBJS Rev, 2018,6(4):e10.
doi: 10.2106/JBJS.RVW.17.00072 |
| [13] |
Reali C, Guy R, Darby CR , et al. Complex reconstruction with flaps after abdominoperineal resection and groin dissection for anal squamous cell carcinoma: adifficult case involving many specialities[J]. Am J Case Rep, 2018,19:61-67.
doi: 10.12659/AJCR.906818 |
| [1] | 崔云鹏,施学东,刘佳,米川,王冰,潘元星,林云飞. 经皮椎弓根螺钉内固定联合可扩张管状牵开器下肿瘤切除治疗脊柱转移瘤的效果[J]. 北京大学学报(医学版), 2023, 55(3): 530-536. |
| [2] | 马利加,胡攀攀,刘晓光. 脊柱转移癌伴软脊膜转移1例[J]. 北京大学学报(医学版), 2023, 55(3): 563-566. |
| [3] | 袁源,郎宁,袁慧书. CT能谱曲线在脊柱转移瘤和感染性病变中的鉴别诊断价值[J]. 北京大学学报(医学版), 2021, 53(1): 183-187. |
| [4] | 张帆,燕太强,郭卫. Rasfonin抑制骨肉瘤细胞143B的增殖和迁移[J]. 北京大学学报(医学版), 2019, 51(2): 234-238. |
| [5] | 马长城,林国中△,王振宇. 颈髓髓内多节段室管膜瘤的早期手术[J]. 北京大学学报(医学版), 0, (): 847-850. |
| [6] | 马长城, 林国中, 王振宇. 颈髓髓内多节段室管膜瘤的早期手术[J]. 北京大学学报(医学版), 2017, 49(5): 847-850. |
| [7] | 闵理,陈春雨,段宏,周勇,张闻力,石锐,罗翼,屠重棋. 骨水泥型同种异体骨复合人工关节治疗股骨近端肿瘤的长期随访[J]. 北京大学学报(医学版), 2016, 48(3): 562-567. |
| [8] | 郭卫, 姬涛. 对脊柱转移癌如何进行合理的治疗[J]. 北京大学学报(医学版), 2015, 47(2): 200-202. |
|
||
