北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (2): 378-381. doi: 10.19723/j.issn.1671-167X.2020.02.029
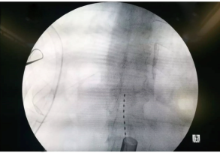
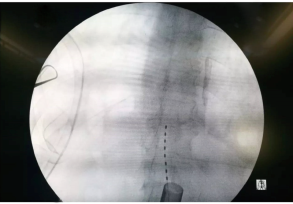
椎间盘镜辅助脊髓刺激电极植入治愈下肢缺血1例
钱亚龙,徐帅,刘海鹰( )
)
- 北京大学人民医院脊柱外科,北京 100044
Lower limb ischemia cured by stimulation electrode implantation assisted with microendoscopic discectomy system: A case report
Ya-long QIAN,Shuai XU,Hai-ying LIU()
- Department of Spinal Surgery, Peking University People's Hospital, Beijing 100044, China
中图分类号:
- R682.6


| [1] | Azab WA, Nasim K, Najibullah M . Lumbar microendoscopic discectomy: surgical technique and nuances[J]. Acta Neurochir (Wien), 2016,158(4):749-753. |
| [2] | 程祝强, 徐霜霜, 金毅 . 脊髓电刺激治疗缺血性肢痛[J]. 国际麻醉学与复苏杂志, 2015,36(7):665-669. |
| [3] | Borjesson M, Andrell P, Mannheimer C . Spinal cord stimulation for long-term treatment of severe angina pectoris: What does the evidence say?[J]. Future Cardiol, 2011,7(6):825-833. |
| [4] | Compton AK, Shah B, Hayek SM . Spinal cord stimulation: A review[J]. Curr Pain Headache Rep, 2012,16(1):35-42. |
| [5] | Fontaine R, Buck P, Riveaux R , et al. Treatment of arterial obli-terations, respective value of thrombectomies and thrombo-end-arteriectomies, of arteriovenous shunts, and of vascular grafts (fresh venous autografts)[J]. Lyon Chir, 1951,46(1):73-94. |
| [6] | 谷涌泉, 张建, 齐立行 , 等. 自体骨髓干细胞移植治疗慢性下肢缺血94例不同病变分期患者的效果比较[J]. 中国临床康复, 2005,9(38):7-10. |
| [7] | Bosiers M, Hart JP, Deloose K , et al. Endovascular therapy as the primary approach for limb salvage in patients with critical limb ischemia: Experience with 443 infrapopliteal procedures[J]. Vascular, 2006,14(2):63-69. |
| [8] | Tendera M, Aboyans V, Bartelink ML , et al. ESC guidelines on the diagnosis and treatment of peripheral artery diseases: Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: the Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2011,32(22):2851-2906. |
| [9] | Guan Y . Spinal cord stimulation: Neurophysiological and neurochemical mechanisms of action[J]. Curr Pain Headache Rep, 2012,16(3):217-225. |
| [10] | Foreman RD, Linderoth B . Neural mechanisms of spinal cord stimulation[J]. Int Rev Neurobiol, 2012,107:87-119. |
| [11] | Wu M, Linderoth B, Foreman RD . Putative mechanisms behind effects of spinal cord stimulation on vascular diseases: A review of experimental studies[J]. Auton Neurosci, 2008,138(1/2):9-23. |
| [12] | Zipes DP, Svorkdal N, Berman D , et al. Spinal cord stimulation therapy for patients with refractory angina who are not candidates for revascularization[J]. Neuromodulation, 2012,15(6):550-559. |
| [13] | Kemler MA ,Barendse GA,van Kleef M,et al.Spinal cord stimulation in patients with chronic reflex sympathetic dystrophy[J]. N Engl J Med, 2000,343(9):618-624. |
| [14] | Taylor RS, van Buyten JP, Buchser E . Spinal cord stimulation for chronic back and leg pain and failed back surgery syndrome: A systematic review and analysis of prognostic factors[J]. Spine (Phila Pa 1976), 2005,30(1):152-160. |
| [15] | 樊碧发 . 脊髓电刺激的镇痛机制及其临床应用[J]. 中华医学信息导报, 2005,20(4):20. |
| [16] | Kleiber JC, Marlier B, Bannwarth M , et al. Is spinal cord stimulation safe? A review of 13 years of implantations and complications[J]. Rev Neurol (Paris), 2016,172(11):689-695. |
| [1] | 李伟浩,张学民,贺致宾,张小明,蒋京军,张韬,李伟,李清乐. 脊髓电刺激术治疗不可手术的慢性严重肢体缺血1例[J]. 北京大学学报(医学版), 2019, 51(2): 362-364. |
|
||
