北京大学学报(医学版) ›› 2021, Vol. 53 ›› Issue (3): 543-548. doi: 10.19723/j.issn.1671-167X.2021.03.017
新型冠状病毒肺炎疫情分级防控水平下北京市发热门诊空间可及性
张佳伟,韩沛恩,杨莉Δ( )
)
- 北京大学公共卫生学院卫生政策与管理系,北京 100191
Spatial accessibility of fever clinics for multi-tiered prevention and control on COVID-19 in Beijing
ZHANG Jia-wei,HAN Pei-en,YANG LiΔ()
- Department of Health Policy and Management, Peking University School of Public Health, Beijing 100191, China
摘要:
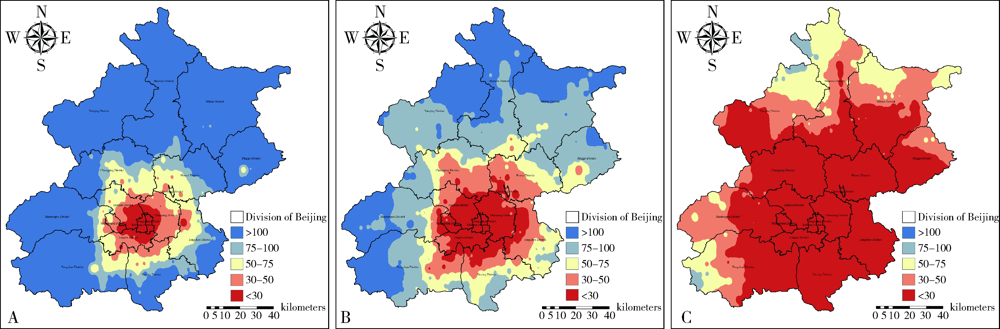
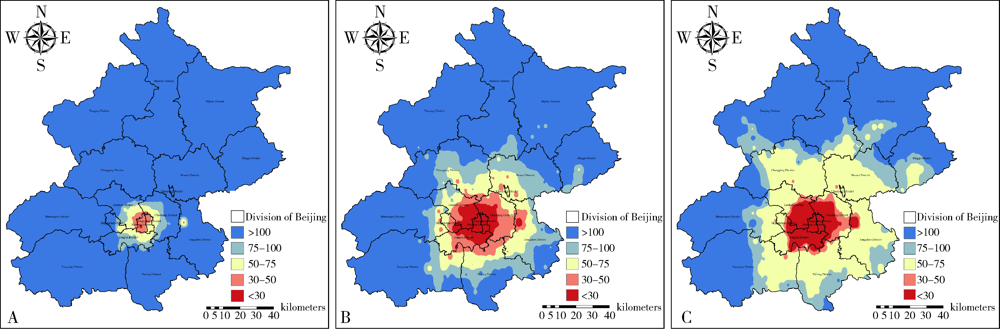
目的: 情景模拟北京市分别作为疫情传播和暴发城市下新型冠状病毒肺炎不同流行程度,并分析北京市发热门诊医疗资源应对能力,为优化北京市重大疫情下医疗资源的空间布局提供科学依据。方法: 应用广义SEIR(susceptible-exposed-infectious-removed)模型进行情景模拟,根据医疗资源、人口流动以及封禁措施等因素预测北京市的新型冠状病毒肺炎流行情况,并应用改进的两步移动搜寻法计算北京市发热门诊的空间可及性现状。结果: 根据SEIR模型模拟得到低、中、高防控水平下北京市作为疫情传播城市单日最高感染人数分别为8 514、183和68例,作为疫情暴发城市单日最高感染人数分别为22 803、10 868和3 725例。北京市模拟为疫情传播城市时,在全市585个居民点中,低防控水平下有17个居民点(2.91%)发热门诊可及性好,41个居民点(7.01%)的发热门诊可及性较好, 56个居民点(9.57%)的发热门诊可及性一般,62个居民点(10.60%)的发热门诊可及性较差,409个居民点(69.91%)发热门诊可及性差;中防控水平下只有房山区西部、门头沟区西部、延庆区北部、怀柔区北部和密云区北部可及性较差;高防控水平下有559个居民点(95.56%)的发热门诊可及性好,24个居民点(4.10%)的发热门诊可及性较好, 2个居民点(0.34%)的发热门诊可及性一般,现有发热门诊可以满足需求。北京市模拟为疫情暴发城市时,低防控水平下仅1个居民点(0.17%)的发热门诊可及性好, 5个居民点(0.86%)的发热门诊可及性较好,10个居民点(1.71%)的发热门诊可及性一般,12个居民点(2.05%)的发热门诊可及性较差, 557个居民点(95.21%)的发热门诊可及性差;中防控和高防控下生态涵养区可及性均较差。结论: 北京市发热门诊资源分布不均。北京市模拟作为疫情传播城市时,高防控水平下可适当减少发热门诊开放数量以避免交叉感染;中等防控水平时开设的发热门诊基本能够满足北京市发热患者的接诊需求,但生态涵养区的发热门诊可及性存在不足,应优先考虑对生态涵养区二级以上公立医院发热门诊进行建设;在防控水平为低时,生态涵养区发热门诊可及性较差,优先考虑生态涵养区发热门诊建设的同时可建立临时发热哨点,缓解门诊压力。北京市模拟作为疫情暴发城市且低防控时由于感染人数较多,需要升级防控水平减少人员流动来遏制疫情发展。
中图分类号:
- R197.2



| [1] | 陈慧, 姜淮芜, 刘静梅. 传染病定点医院新冠肺炎疫情期间发热门诊分区分级接诊策略[J]. 寄生虫病与感染性疾病, 2020,18(3):141-144. |
| [2] | Noll NB, Aksamentov I, Druelle V, et al. COVID-19 scenarios: an interactive tool to explore the spread and associated morbidity and mortality of SARS-CoV-2[J]. (2020-05-12)[2020-12-20]. https://doi.org/10.1101/2020.05.05.20091363. |
| [3] |
Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia[J]. N Engl J Med, 2020,382(13):1199-1207.
doi: 10.1056/NEJMoa2001316 |
| [4] | 中国疾病预防控制中心. 新型冠状病毒肺炎流行病学特征分析[J]. 中华流行病学杂志, 2020,41(2):145-151. |
| [5] | Yang Y, Lu QB, Liu MJ, et al. Epidemiological and clinical features of the 2019 novel coronavirus outbreak in China[J]. (2020-02-21)[2020-11-21]. https://doi.org/10.1101/2020.02.10.20021675 |
| [6] | Qin J, You C, Lin Q, et al. Estimation of incubation period distribution of COVID-19 using disease onset forward time: A novel cross-sectional and forward follow-up study[J]. Sci Adv, 2020,6(33):1202. |
| [7] |
Pan A, Liu L, Wang C, et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China[J]. JAMA, 2020,323(19):1915-1923.
doi: 10.1001/jama.2020.6130 pmid: 32275295 |
| [8] |
Wang F. Why public health needs GIS: a methodological overview[J]. Ann GIS, 2020,26(1):1-12.
doi: 10.1080/19475683.2019.1702099 |
| [9] |
Mcgrail MR. Spatial accessibility of primary health care utilising the two step floating catchment area method: an assessment of recent improvements[J]. Int J Health Geogr, 2012,11:50.
doi: 10.1186/1476-072X-11-50 |
| [10] |
Luo W, Qi Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians[J]. Health Place, 2009,15(4):1100-1107.
doi: 10.1016/j.healthplace.2009.06.002 |
| [11] |
陶卓霖, 程杨. 两步移动搜寻法及其扩展形式研究进展[J]. 地理科学进展, 2016,35(5):589-599.
doi: 10.18306/dlkxjz.2016.05.006 |
| [12] |
Wang X, Yang H, Duan Z, et al. Spatial accessibility of primary health care in China: a case study in Sichuan Province[J]. Soc Sci Med, 2018,209:14-24.
doi: 10.1016/j.socscimed.2018.05.023 |
| [13] |
Wang X, Pan J. Assessing the disparity in spatial access to hospital care in ethnic minority region in Sichuan Province, China[J]. BMC Health Serv Res, 2016,16(1):399.
doi: 10.1186/s12913-016-1643-8 |
| [14] |
Vadrevu L, Kanjilal B. Measuring spatial equity and access to maternal health services using enhanced two step floating catchment area method (E2SFCA): a case study of the Indian Sundarbans[J]. Int J Equity Health, 2016,15(1):87.
doi: 10.1186/s12939-016-0376-y |
| [15] |
Nakamura T, Nakamura A, Mukuda K, et al. Potential accessibi-lity scores for hospital care in a province of Japan: GIS-based ecological study of the two-step floating catchment area method and the number of neighborhood hospitals[J]. BMC Health Serv Res, 2017,17(1):438.
doi: 10.1186/s12913-017-2367-0 pmid: 28651532 |
| [16] |
Tao Z, Cheng Y, Zheng Q, et al. Measuring spatial accessibility to healthcare services with constraint of administrative boundary: a case study of Yanqing District, Beijing, China[J]. Int J Equity Health, 2018,17(1):7.
doi: 10.1186/s12939-018-0720-5 |
| [17] | 陶卓霖, 程杨, 戴特奇, 等. 公共服务设施布局优化模型研究进展与展望[J]. 城市规划, 2019,43(8):60-68, 88. |
| [18] | 程敏, 黄维维. 基于高斯两步移动搜索法的上海市养老设施空间可达性评价[J]. 复旦学报(自然科学版), 2020,59(2):129-136. |
| [19] |
Cheng G, Zeng X, Duan L, et al. Spatial difference analysis for accessibility to high level hospitals based on travel time in Shenzhen, China[J]. Habitat Int, 2016,53:485-494.
doi: 10.1016/j.habitatint.2015.12.023 |
| [20] |
Peeters D, Thomas I. Distance predicting functions and applied location-allocation models[J]. J Geogr Syst, 2000,2(2):167-184.
doi: 10.1007/PL00011453 |
| [21] |
Siegel M, Koller D, Vogt V, et al. Developing a composite index of spatial accessibility across different health care sectors: A German example[J]. Health Policy, 2016,120(2):205-212.
doi: 10.1016/j.healthpol.2016.01.001 |
| [22] | 中共北京市委办公厅, 北京市人民政府办公厅. 关于印发《加强首都公共卫生应急管理体系建设三年行动计划(2020—2022年)》的通知[J]. 北京市人民政府公报, 2020(32):26-47. |
| [23] | 左克强, 金逸, 焦岳龙, 等. 新冠肺炎疫情后发热门诊及门急诊诊疗流程优化之策[J]. 中国医院院长, 2020,16(21):81-83. |
| [1] | 张佳伟, 朱正, 巩超, 韩润之, 杨莉. 北京市儿科医疗资源空间可及性与优化[J]. 北京大学学报(医学版), 2026, 58(3): 472-478. |
|
||
