北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (4): 669-673. doi: 10.19723/j.issn.1671-167X.2022.04.014
中危非肌层浸润性膀胱癌的最佳膀胱镜监测强度
王飞,秦彩朋,杜依青,刘士军,李清,徐涛*( )
)
- 北京大学人民医院泌尿外科,北京 100044
Optimal surveillance intensity of cystoscopy in intermediate-risk non-muscle invasive bladder cancer
Fei WANG,Cai-peng QIN,Yi-qing DU,Shi-jun LIU,Qing LI,Tao XU*()
- Department of Urology, Peking University People's Hospital, Beijing 100044, China
摘要:
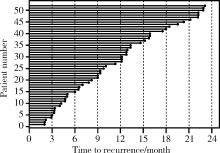
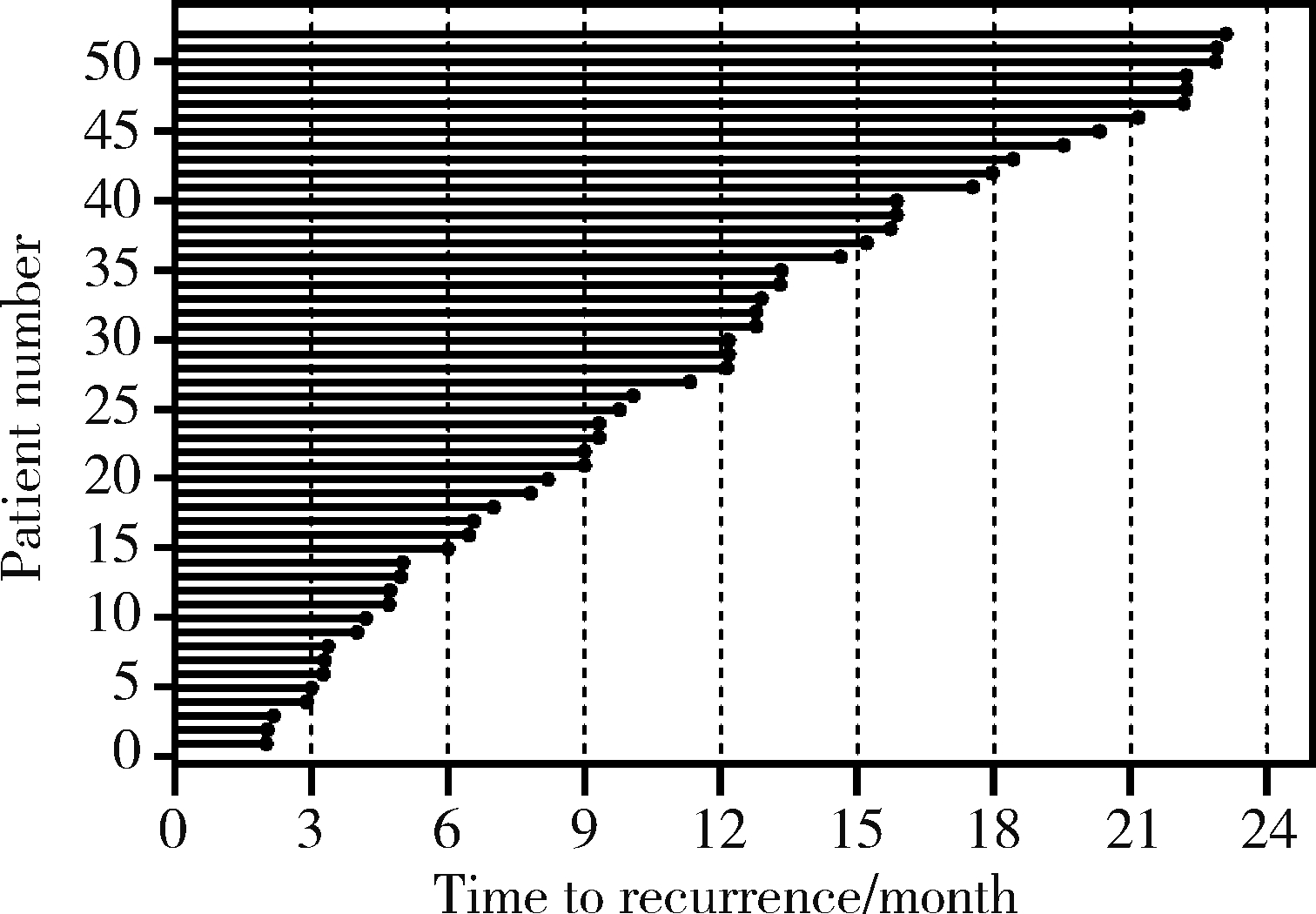
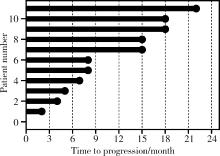
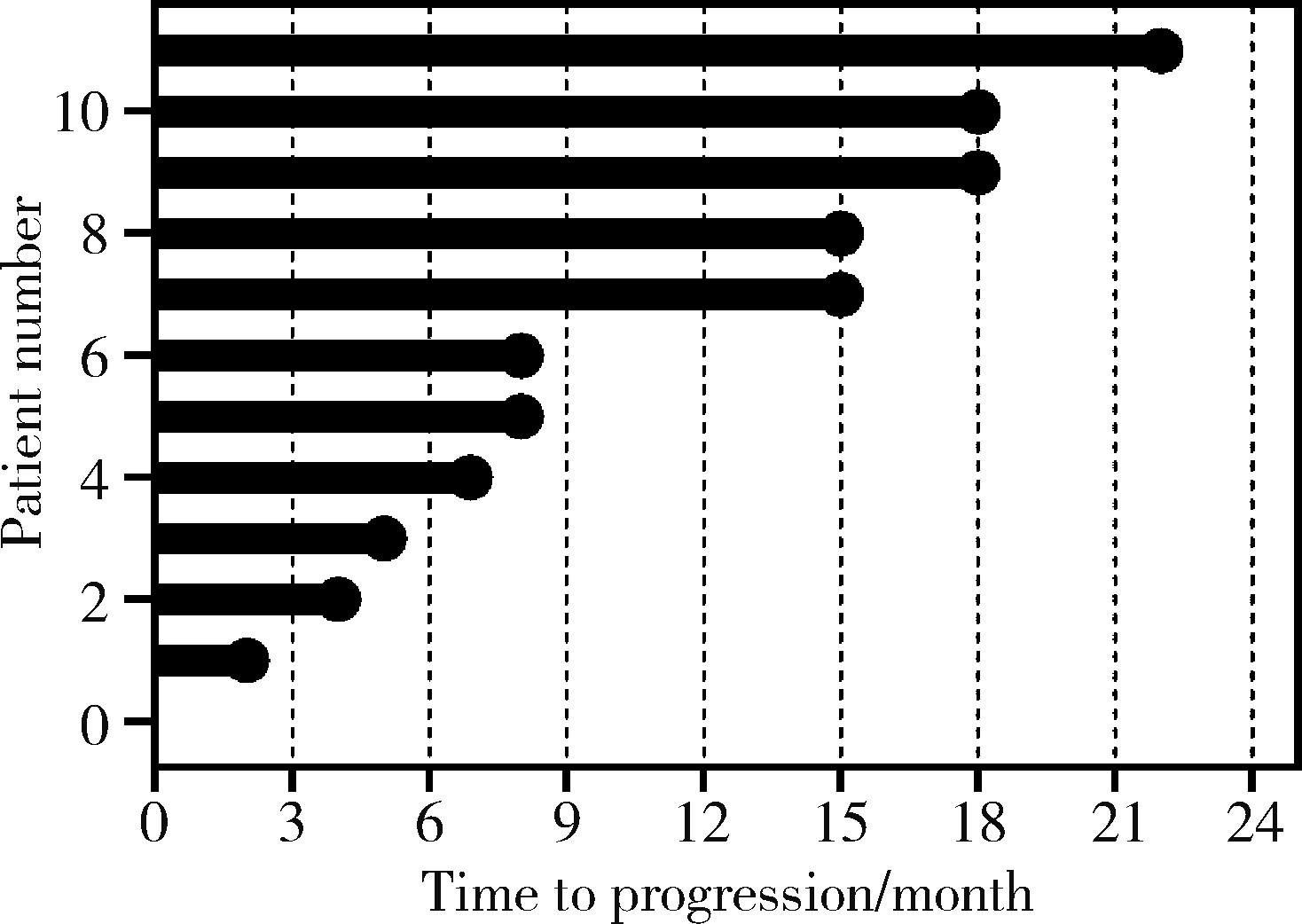
目的: 为中危非肌层浸润性膀胱癌确定最佳的膀胱镜监测频率方法: 回顾性分析2001年1月至2019年10月于北京大学人民医院行经尿道膀胱肿瘤电切术的中危非肌层浸润性膀胱癌患者,收集患者的临床、病理学和随访资料。术后2年每3至6个月对患者进行膀胱镜检测,根据患者复发和进展的情况,在术后2年假设3种强度的监测策略:模式1:间隔3个月,模式2:间隔6个月,模式3:间隔12个月,比较3种模式间检测复发和进展的延迟个数和时间差异。结果: 共纳入185例患者,其中男性144例(77.8%),女性41例(22.2%),中位年龄68 (59~76)岁。单发肿瘤有118例(63.8%),多发肿瘤有67例(36.2%)。术后病理Ta期179例(96.8%),T1期有6例(3.2%)。高级别病变108例(58.4%),低级别病变77例(41.6%)。在术后2年随访期间内,52例(28.1%)患者出现复发,133例(71.9%)未出现复发;11例(5.9%)患者发生进展,174例(94.1%)未发生进展。相比于模式1,模式2出现复发检测延迟的个数为29例(55.8%),模式3为41例(78.8%),两者之间差异有统计学意义(P=0.012)。模式1、模式2和模式3检测复发的中位延迟时间分别为1.00、1.99和4.19个月。模式1与模式2和模式3之间差异均有统计学意义(P=0.001, P=0.013)。与模式1相比,模式2出现进展检测延迟的个数为5例(45.4%),模式3为8例(72.7%),两者之间差异无统计学意义。模式1、模式2和模式3检测进展的中位延迟时间分别为1.00、2.00和3.00个月,三者之间差异无统计学意义。结论: 6个月间隔的膀胱镜检测模式与3个月相比,虽然会稍微延迟检测到肿瘤复发和进展,但不会造成严重的不良结局,并能够减少患者的痛苦和经济负担,在中危非肌层浸润性膀胱癌是可行的。
中图分类号:
- R737.1
| 1 | 李辉章, 郑荣寿, 杜灵彬, 等. 中国膀胱癌流行现状与趋势分析[J]. 中华肿瘤杂志, 2021, 43 (3): 6. |
| 2 | 陈晓芳, 陈万青, 周薇薇, 等. 2013年中国膀胱癌发病和死亡流行状况分析[J]. 中国肿瘤, 2018, 27 (2): 5. |
| 3 |
Kamat AM , Hahn NM , Efstathiou JA , et al. Bladder cancer[J]. Lancet, 2016, 388 (10061): 2796.
doi: 10.1016/S0140-6736(16)30512-8 |
| 4 |
Babjuk M , Burger M , Compérat EM , et al. European association of urology guidelines on non-muscle-invasive bladder cancer (TaT1 and carcinoma in situ): 2019 update[J]. Eur Urol, 2019, 76 (5): 639- 657.
doi: 10.1016/j.eururo.2019.08.016 |
| 5 |
Rhijn B , Burger M , Lotan Y , et al. Recurrence and progression of disease in non-muscle-invasive bladder cancer: from epidemio-logy to treatment strategy[J]. Eur Urol, 2009, 56 (3): 430- 442.
doi: 10.1016/j.eururo.2009.06.028 |
| 6 |
Burger M , Catto JW , Dalbagni G , et al. Epidemiology and risk factors of urothelial bladder cancer[J]. Eur Urol, 2013, 63 (2): 234- 241.
doi: 10.1016/j.eururo.2012.07.033 |
| 7 |
Chang SS , Boorjian SA , Chou R , et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline[J]. J Urol, 2016, 196 (4): 1021- 1029.
doi: 10.1016/j.juro.2016.06.049 |
| 8 |
Ritch CR , Velasquez MC , Kwon D , et al. Use and validation of the AUA/SUO risk grouping for nonmuscle invasive bladder cancer in a contemporary cohort[J]. J Urol, 2020, 203 (3): 505- 511.
doi: 10.1097/JU.0000000000000593 |
| 9 |
Han C , Mengual L , Kang B , et al. Validation of urine-based gene classifiers for detecting bladder cancer in a chinese study[J]. J Cancer, 2018, 9 (17): 3208- 3215.
doi: 10.7150/jca.24506 |
| 10 |
Zhu CZ , Ting HN , Ng KH , et al. A review on the accuracy of bladder cancer detection methods[J]. J Cancer, 2019, 10 (17): 4038- 4044.
doi: 10.7150/jca.28989 |
| 11 |
Nielsen ME , Smith AB , Meyer AM , et al. Trends in stage-specific incidence rates for urothelial carcinoma of the bladder in the United States: 1988 to 2006[J]. Cancer, 2014, 120 (1): 86- 95.
doi: 10.1002/cncr.28397 |
| 12 | Martin DT , Shen H , Steinbach-Rankins JM , et al. Glycoprotein-130 expression is associated with aggressive bladder cancer and is a potential therapeutic target[J]. Mol Cancer Ther, 2018, 18 (2): 413- 420. |
| 13 |
Mason SJ , Downing A , Wright P , et al. Health-related quality of life after treatment for bladder cancer in England[J]. Br J Can-cer, 2018, 118 (11): 1518- 1528.
doi: 10.1038/s41416-018-0084-z |
| 14 |
Kamat AM , Witjes JA , Brausi M , et al. Defining and treating the spectrum of intermediate risk nonmuscle invasive bladder cancer[J]. J Urol, 2014, 192 (2): 305- 315.
doi: 10.1016/j.juro.2014.02.2573 |
| 15 |
Bhat A , Kwon D , Soodana-Prakash N , et al. Surveillance intensity in intermediate risk nonmuscle invasive bladder cancer: revisiting the optimal timing and frequency of cystoscopy[J]. J Urol, 2021, 206 (1): 22- 28.
doi: 10.1097/JU.0000000000001689 |
| 16 |
Soria F , D'Andrea D , Abufaraj M , et al. Stratification of intermediate-risk non-muscle-invasive bladder cancer patients: implications for adjuvant therapies[J]. Eur Urol Focus, 2021, 7 (3): 566- 573.
doi: 10.1016/j.euf.2020.05.004 |
| 17 |
Kohada Y , Ha Yashi T , Hsi RS , et al. Recurrence and progression free survival of intermediate risk non-muscle invasive bladder cancer: the impact of conditional evaluation and sub-classification[J]. BJU Int, 2021, 127 (4): 473- 485.
doi: 10.1111/bju.15209 |
| 18 |
Fukushima H , Moriyama S , Waseda Y , et al. Significance of bladder neck involvement in risk substratification of intermediate-risk non-muscle-invasive bladder cancer[J]. Eur Urol Focus, 2021, 7 (2): 366- 372.
doi: 10.1016/j.euf.2020.01.006 |
| 19 |
Reyes RM , Rios E , Barney S , et al. A randomized feasibility trial comparing surveillance regimens for patients with low and low-intermediate risk non-muscle invasive bladder cancer[J]. Bladder Cancer, 2021, 7 (3): 285- 295.
doi: 10.3233/BLC-201535 |
| 20 | Wallace D , Bryan RT , Dunn JA , et al. Delay and survival in bladder cancer[J]. BJU Int, 2015, 89 (9): 868- 878. |
| [1] | 李慎谟, 苏丹丹, 林己煜, 宋昊东, 马潞林, 侯小飞, 王国良, 张洪宪, 叶剑飞, 张树栋. 腹腔镜下膀胱癌根治术同期行肾输尿管全长切除术的预后分析[J]. 北京大学学报(医学版), 2025, 57(5): 961-966. |
| [2] | 缪祺, 洪保安, 张学舟, 孙志鹏, 王维, 王宇轩, 薄予轩, 赵佳晖, 张宁. 膀胱癌合并冠心病患者行经尿道膀胱肿瘤切除术围手术期抗血小板药物管理[J]. 北京大学学报(医学版), 2025, 57(4): 698-703. |
| [3] | 刘欢锐,彭祥,李森林,苟欣. 基于HER-2相关基因构建风险模型用于膀胱癌生存预后评估[J]. 北京大学学报(医学版), 2023, 55(5): 793-801. |
| [4] | 戴翔,左美妮,张晓鹏,胡浩,徐涛. 经皮肾镜术中不同憩室颈部处理方式治疗肾盏憩室结石的长期预后[J]. 北京大学学报(医学版), 2021, 53(4): 704-709. |
| [5] | 王明瑞,王起,胡浩,赖金惠,贺永新,熊杰,刘献辉,刘士军,许克新,徐涛. 标准通道经皮肾镜取石术治疗孤立肾肾结石的长期安全性和有效性[J]. 北京大学学报(医学版), 2020, 52(4): 663-666. |
| [6] | 李玉慧,苏波,林福安,费雅楠,于笑霞,范文强,陈海英,张学武,贾园. 银屑病关节炎患者就医行为及治疗现状的多中心调查[J]. 北京大学学报(医学版), 2019, 51(6): 1014-1018. |
| [7] | 杨飞龙,洪锴,赵国江,刘承,宋一萌,马潞林. 基于长链非编码RNA的生物信息学分析构建膀胱癌预后模型并确定预后生物标志物[J]. 北京大学学报(医学版), 2019, 51(4): 615-622. |
| [8] | 黄海文,闫兵,尚美霞,刘漓波,郝瀚,席志军. 女性膀胱癌患者腹腔镜膀胱全切术与开放膀胱全切术的倾向性评分匹配比较[J]. 北京大学学报(医学版), 2019, 51(4): 698-705. |
| [9] | 覃子健,毕海,马潞林,黄毅,张帆. 肠代膀胱内原发肠源性腺癌1例[J]. 北京大学学报(医学版), 2018, 50(4): 737-739. |
| [10] | 唐兴国,颜野,邱敏,卢剑,陆敏,侯小飞,黄毅,马潞林. 单中心16年青年膀胱尿路上皮癌患者的诊治[J]. 北京大学学报(医学版), 2018, 50(4): 630-633. |
| [11] | 张海东,张立,释栋,韩劼,闫夏,谢也斯,孟焕新. 锥形锁柱种植体用于因牙周炎缺牙患者修复的临床观察[J]. 北京大学学报(医学版), 2018, 50(2): 300-307. |
| [12] | 叶海云,许清泉,黄晓波,马凯,王晓峰. 卡介苗膀胱灌注治疗致结核性前列腺脓肿1例[J]. 北京大学学报(医学版), 2015, 47(6): 1039-1041. |
| [13] | 姚林, 张雷, 范宇, 张政, 徐燕鹏, 刘茗洁, 何志嵩, 龚侃, 李学松, 张争, 张崔健, 周利群. 前瞻随机对照研究:新技术对硬性膀胱镜患者舒适度的提高[J]. 北京大学学报(医学版), 2014, 46(4): 635-637. |
| [14] | 沈棋, 胡帅, 李峻, 王静华, 何群. 膀胱前列腺切除术中前列腺偶发癌发生率及临床病理特点分析[J]. 北京大学学报(医学版), 2014, 46(4): 515-518. |
| [15] | 邵光军,蔡林,李学松,宋刚,李雪迎,何志嵩,周利群. 脐尿管癌:单中心30年经验总结[J]. 北京大学学报(医学版), 2013, 45(5): 774-778. |
|
||
