
婴儿过敏性肠炎是临床较常见的过敏性疾病,主要是由于摄入外源蛋白产生免疫介导反应并引起的结肠、直肠炎性改变,一般以牛奶蛋白过敏多见,还有少数为鸡蛋、花生等过敏[1-2]。牛奶蛋白过敏性肠炎婴儿多表现为呕吐、腹痛、腹胀等消化道症状。与鸡蛋、花生过敏相比,牛奶蛋白过敏性肠炎症状无特异性,尤其是早期发作且未做过敏原筛查的婴儿,容易出现漏诊、误诊,并且婴儿的依从性不高,可能会影响临床诊断[3-4]。嗜酸性粒细胞(eosinophilic granulocytes,EOS)是反映炎症反应的常规指标,血小板(platelets,PLT)是临床常用血常规检测指标,已有研究证实二者在婴儿过敏性肠炎中具有较好的诊断价值,但是目前这两种指标通用于诊断婴儿过敏性肠炎,并不会区别具体过敏原,因此对能否作为诊断牛奶蛋白过敏原引起的过敏性肠炎的诊断工具,仍需要进一步研究[5]。除此之外,钙卫蛋白是由S100A8和S100A9两种蛋白质形成的异二聚体,广泛存在于人体组织,粪便钙卫蛋白多由肠道中性粒细胞释放,其性质稳定、不易分解且易于测量,可反映肠道炎症程度,本课题组推测粪便钙卫蛋白可能成为胃肠道炎症的有效标志物[6-8]。但钙卫蛋白在牛奶蛋白过敏性肠炎与非牛奶蛋白过敏性肠炎临床鉴别中的效能仍尚需评估。基于此,本研究旨在分析粪便钙卫蛋白能否作为诊断牛奶蛋白过敏原引起的过敏性肠炎的诊断指标,探讨粪便钙卫蛋白对牛奶蛋白过敏性肠炎婴儿的诊断价值,以提高牛奶蛋白过敏性肠炎临床诊断准确率。
1 资料与方法
1.1 婴儿基本资料
选择2020年1月至2023年1月在杭州市儿童医院就诊的87例过敏性肠炎婴儿的病例资料进行回顾性分析,将确诊为牛奶蛋白过敏性肠炎的38例婴儿设为A组,非牛奶蛋白过敏性肠炎的49例婴儿设为B组,再收集同期健康婴儿73例设为C组。本研究开始前已经杭州市儿童医院医学伦理委员会审查批准[2019年伦理(临研)第(12)号],所有参与研究婴儿的监护人均签署知情同意书。
1.2 纳入及排除标准
A组纳入标准:(1)符合《食物过敏相关消化道疾病诊断与管理专家共识》诊断标准,并伴有呕吐或腹泻等症状[9];(2)牛奶蛋白回避-口服激发试验阳性;(3)婴儿年龄3~10个月。B组纳入标准: (1)临床症状符合过敏性肠炎[9];(2)牛奶蛋白回避-口服激发试验阴性;(3)年龄3-10个月。C组纳入标准: (1)未患过敏性肠炎;(2)年龄3~10个月;(3)婴儿一般情况良好,无特异性皮炎或湿疹;(4)无其他过敏史。排除标准: (1)其他肠道出血性疾病、肠道感染性疾病、早发炎症性肠病者;(2)血液系统疾病者;(3)过敏性紫癜者;(4)免疫功能障碍者;(5)凝血功能障碍者;(6)肝、肾等重要脏器功能不全者;(7)临床资料不全者。
1.3 研究方法
收集所有婴儿一般资料(包括性别、病程、年龄、喂养方式)和实验室检查结果(包括白细胞、血红蛋白、EOS、PLT);收集所有婴儿粪便钙卫蛋白指标,保存3组婴儿的10~20 g粪便标本,接种环挑取粪便标本50~100 mg,按照体积比1 ∶ 49加入萃取液,充分混匀后,取2 mL均浆移入离心管,10 000 r/min离心5 min,取上清液-20 ℃保存,采用免疫层析法检测粪便钙卫蛋白水平,试剂盒购自湖南省丽拓生物科技有限公司。
1.4 统计学分析
使用SPSS 20.0软件,计数资料以n(%)表示,两组间比较采用卡方检验,分类变量比较采用卡方检验,采用Shapiro-Wilk检验计量资料正态性,服从正态分布的计量资料以$\bar x \pm s$表示,3组间各指标比较采用单因素方差分析,组间两两比较采用LSD检验;不服从正态分布的计量资料以M(P25,P75)表示,组间比较采用秩和检验,并采用受试者工作特征(receiver operating characteristic,ROC)曲线下面积(area under characteristic,AUC)分析粪便钙卫蛋白的诊断价值,采用Pearson法分析EOS、PLT水平与粪便钙卫蛋白水平的相关性,P < 0.05认为差异具有统计学意义。
2 结果
3组婴儿间性别、病程、年龄、喂养方式、白细胞、血红蛋白比较差异均无统计学意义(P>0.05);A组EOS、PLT水平高于B组、C组(P < 0.05),B组高于C组(P < 0.05,表 1)。
表1 3组婴儿一般资料比较Table 1 Comparison of general data in three groups |
| Group | n | Gender,n(%) | Course of the disease/months,M(P25, P75) | Age/months, M(P25, P75) | Feeding methods,n(%) | White blood cell/(×109 /L), M(P25,P75) | Hemoglobin/(g/L), M(P25,P75) | EOS/(×109 L),$\bar x \pm s$ | PLT/(×109 L),$\bar x \pm s$ | |||
| Male | Female | Exclusive breastfeeding | Artificial feeding | Mixed feeding | ||||||||
| A | 38 | 21 (55) | 17 (45) | 4.00 (3.00, 6.00) | 5.50 (4.00, 7.75) | 12 (32) | 8 (21) | 18 (47) | 8.50 (8.00, 9.00) | 115.50 (112.25, 118.00) | 0.73±0.21 | 381.03±46.04 |
| B | 49 | 22 (45) | 27 (55) | 5.00 (3.00, 6.00) | 6.00 (5.00, 7.00) | 16 (33) | 12 (24) | 21 (43) | 8.00 (8.00, 9.00) | 114.00 (112.00, 118.00) | 0.41±0.10* | 336.98±52.57* |
| C | 73 | 40 (55) | 33 (45) | 5.00 (3.00, 5.00) | 6.00 (5.00, 7.00) | 23 (32) | 11 (15) | 39 (53) | 9.00 (8.00, 9.00) | 116.00 (112.00, 119.00) | 0.26±0.05*# | 300.22±23.00*# |
| F/H/χ2 | 1.379 | 0.473 | 1.086 | 2.120 | 0.378 | 0.846 | 188.977 | 52.298 | ||||
| P | 0.502 | 0.789 | 0.581 | 0.714 | 0.828 | 0.655 | < 0.001 | < 0.001 | ||||
*P < 0.05, compared with group A; # P < 0.05, compared with group B. EOS, eosinophilic granulocytes; PLT, platelets. |
A组粪便钙卫蛋白水平[(324.45±174.56) μg/g]高于B组[(196.12±83.39) μg/g]和C组[(143.73±50.54) μg/g](P < 0.05),B组粪便钙卫蛋白水平高于C组(P < 0.05)。
EOS水平与粪便钙卫蛋白水平呈正相关(r=0.325,P < 0.001);PLT水平与粪便钙卫蛋白水平呈正相关(r=0.280,P < 0.001)。
3 讨论
为降低牛奶蛋白过敏性肠炎婴儿误诊率,本研究发现粪便钙卫蛋白在牛奶蛋白过敏性肠炎婴儿中可能有较高的诊断价值。婴儿早期免疫系统未发育完全,肠道稳态处于不平衡状态,胃肠道黏膜屏障功能不成熟,肠壁通透性高,肠道内蛋白吸收量增加,过敏原进入肠道概率上升,易出现炎症反应[10]。EOS、PLT是临床常用炎症检测指标,其水平上升表明炎症反应加剧。有研究表明[5],牛奶蛋白过敏性肠炎患儿EOS、PLT指标水平明显上升。还有学者提出,粪便钙卫蛋白主要来源于肠道黏膜层,其水平变化与消化道内炎症程度相关,水平越高说明炎症反应越严重[11]。本研究显示,与非牛奶蛋白过敏性婴儿和健康婴儿相比,牛奶蛋白过敏性婴儿粪便钙卫蛋白水平较高,分析其原因可能是钙卫蛋白主要来源于中性粒细胞和巨噬细胞,属于保护性蛋白质,当机体发生炎症性肠病,细胞发生破裂或死亡时,会被大量释放于肠道,且其具有较强的抗热性和抗蛋白酶活性,难以被细菌和溶菌酶分解,稳定性强,故在过敏性肠炎婴儿粪便中水平较高[12-13]。Lacy等[14]研究表明,IBD患儿病变黏膜中的中性粒细胞能够分泌大量的钙卫蛋白,使其血浆浓度明显升高,与本研究结果一致,进一步说明钙卫蛋白与肠道炎症密切相关。本研究通过对比3组间粪便钙卫蛋白水平,可验证粪便钙卫蛋白能否有效区分“疾病状态”与“健康状态”,并初步探查其鉴别“过敏性”与“非过敏性”肠炎的能力。
本研究还通过分析EOS、PLT水平与粪便钙卫蛋白水平的相关性,探究肠道局部炎症与炎症反应之间的内在联系,从而为理解疾病病理生理机制提供线索,并初步评估粪便钙卫蛋白作为炎症严重程度间接标志物的潜力。相关性研究显示,EOS、PLT水平与粪便钙卫蛋白水平呈正相关,推测粪便钙卫蛋白水平可作为肠道炎症程度的有效指标,牛奶蛋白过敏性肠炎婴儿EOS、PLT水平越高,体内炎症反应越严重,释放的钙卫蛋白就越多。虽然EOS、PLT水平与粪便钙卫蛋白水平之间存在统计学上的显著正相关,但其相关系数(r值分别为0.325和0.280)均较小,表明仅存在弱相关性,可能不具备明确的诊断价值,考虑可能与本研究样本量较少有关,后续工作应着力于扩大样本量,并采用更精细的研究设计,以进一步使研究结果更具说服力。
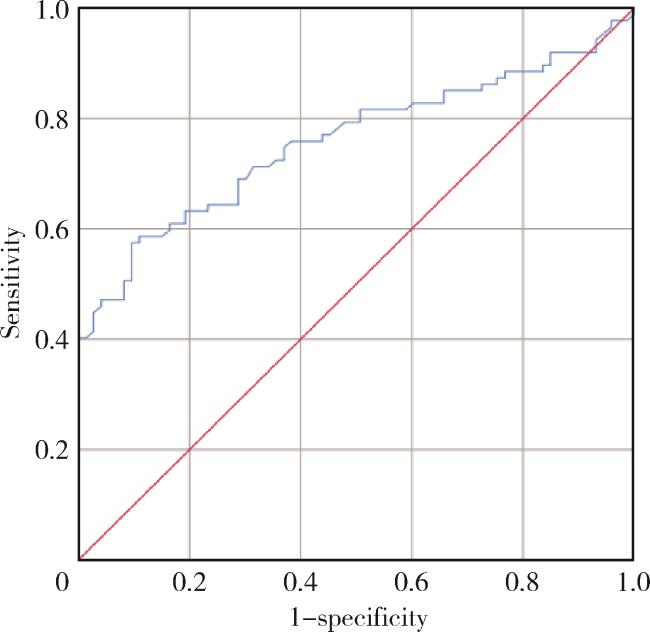
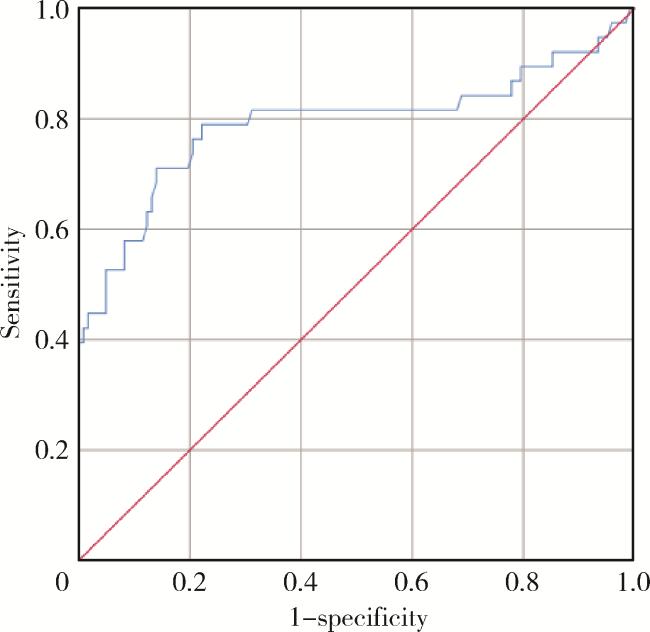
本研究通过检测所有疑似牛奶蛋白过敏性肠炎婴儿及健康婴儿EOS、PLT与粪便钙卫蛋白水平,计算得出粪便钙卫蛋白对过敏性肠炎、牛奶蛋白过敏性肠炎均有较高的诊断价值,且对牛奶蛋白过敏性肠炎诊断准确率较高。通过ROC曲线,可评估粪便钙卫蛋白对过敏性肠炎的诊断价值,并有效鉴别牛奶蛋白过敏性肠炎和非牛奶蛋白过敏性肠炎婴儿,为解决上述临床鉴别诊断难题提供量化依据。但本研究中样本来源单中心且例数有限,研究结果不足以代表所有牛奶蛋白过敏性肠炎婴儿情况,这表明目前对其诊断效能的证据尚属初步,不足以支撑有确定意义的临床价值,粪便钙卫蛋白指标诊断效能还需未来更大样本、多中心研究进一步探索。
综上所述,粪便钙卫蛋白在牛奶蛋白过敏性肠炎婴儿中可能有较高的诊断价值,且EOS、PLT水平与粪便钙卫蛋白水平呈正相关,粪便钙卫蛋白水平越高,炎症反应越严重。

{kind=link}
{kind=link}
{kind=link}
{kind=link}