Journal of Peking University(Health Sciences) ›› 2020, Vol. 52 ›› Issue (1): 97-102. doi: 10.19723/j.issn.1671-167X.2020.01.015
Previous Articles Next Articles
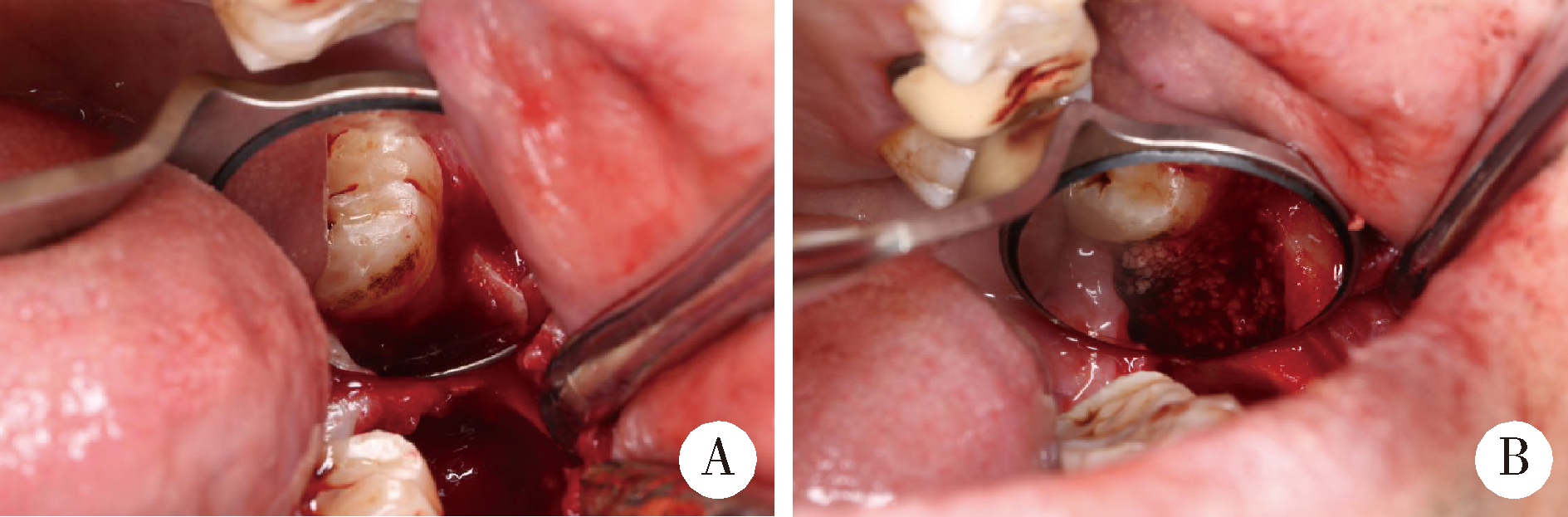
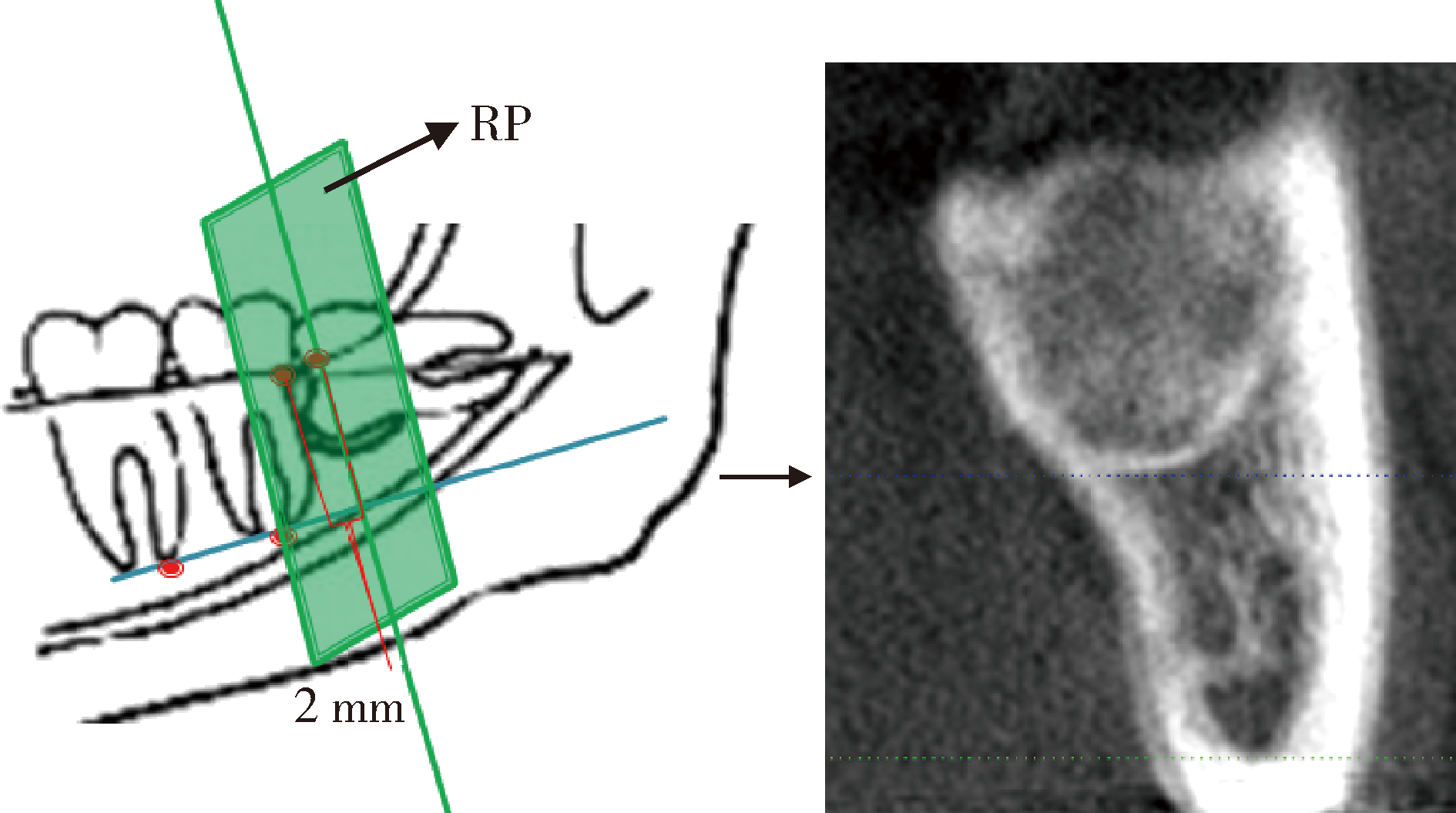
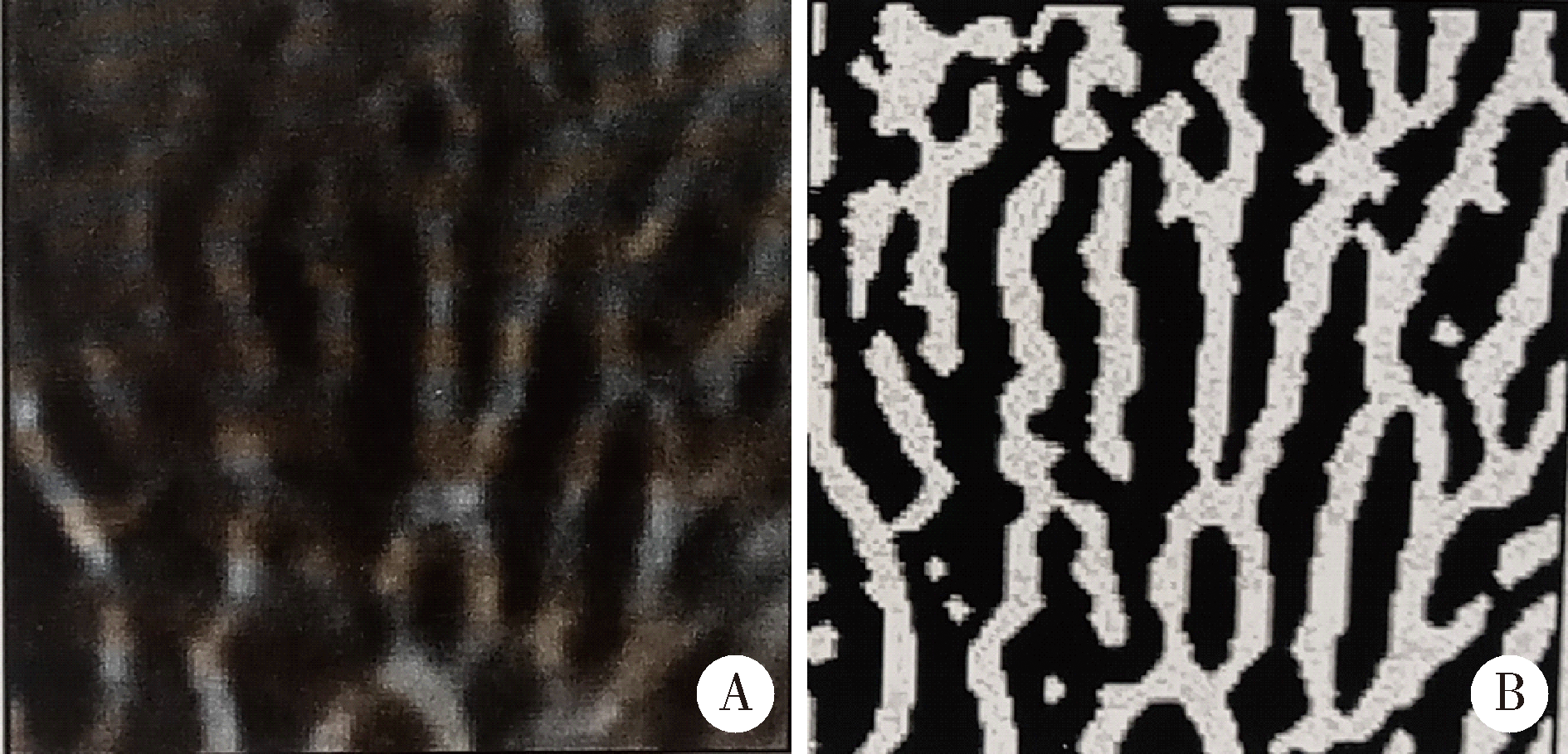
Application of β-TCP for bone defect restore after the mandibular third molars extraction: A split-mouth clinical trial
Chang CAO,Fei WANG,En-bo WANG( ),Yu LIU()
),Yu LIU()
- Department of Oral and Maxillofacial Surgery, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
CLC Number:
- R782.1






| [1] | Kugelberg CF . Impacted lower third molars and periodontal health. An epidemiological, methodological, retrospective and prospective clinical study[J]. Swed Dent J Suppl, 1990,68:1-52. |
| [2] | Martin R, Louvrier A, Meyer C . Consequences of impacted wisdom teeth extraction on the periodontal environment of second molars, a pilot study[J]. J Stomatol Oral Maxillofac Surg, 2017,118(2):78-83 |
| [3] | Hassan KS, Marei HF, Alagl AS . Does grafting of third molar extraction sockets enhance periodontal measures in 30- to 35-year-old patients[J]. J Oral Maxillofac Surg, 2012,70(4):757-764. |
| [4] | Kanr P, Maria A . Eficacy of platelet rich plasma and hydroxyapatite crystals in bone regeneration after surgical removal of mandibular third molars[J]. Maxillofac Oral Surg, 2013,12(1):51-59. |
| [5] | Barbato L, Kalemaj Z, Buti J , et al. Effect of surgical intervention for removal of mandibular third molar on periodontal healing of adjacent mandibular second molar: a systematic review and bayesian network meta-analysis[J]. J Periodontol, 2016,87(3):291-302. |
| [6] | Tabrizi R . Use of lincomycin-impregnated demineralized freeze-dried bone allograft in the periodontal defect after third molar surgery[J]. J Oral Maxillofac Surg, 2014,72(5):850-857. |
| [7] | 刘树铭, 张祖燕, 李居朋 , 等. 健康青年人髁突松质骨结构锥形束CT分析[J]. 中华口腔医学杂志, 2007,42(6):357-360. |
| [8] | Kan KW, Liu JK, Lo EC , et al. Residual periodontal defects distal to the mandibular second molar 6-36 months after impacted third molar extraction[J]. J Clin Periodontol, 2002,29(11):1004-1011. |
| [9] | Leung WK, Corbet EF, Kan KW , et al. A regimen of systematic periodontal care after removal of impacted mandibular third molars manages periodontal pockets associated with the mandibular second molars[J]. J Clin Periodontol, 2005,32(7):725-731. |
| [10] | Qu HL, Tian BM, Chen FM , et al. Effect of asymptomatic visible third molars on periodontal health of adjacent second molars: a cross-sectional study.[J] J Oral Maxillofac Surg, 2017,75(10):2048-2057 |
| [11] | Faria AI, Gallas-Torreira M, Lσpez-Ratσn M . Mandibular second molar periodontal healing after impacted third molar extraction in young adults[J]. J Oral Maxillofac Surg, 2012,70(12):2732-2741. |
| [12] | Zimmerer RM, Jehn P, Kokemüller H , et al. In vivo tissue engineered bone versus autologous bone: stability and structure[J]. Int J Oral Maxillofac Surg, 2017,46(3):385-393. |
| [13] | Jensen T, Schou S, Stavropoulos A , et al. Maxillary sinus floor augmentation with Bio-Oss or Bio-Oss mixed with autogenous bone as graft: a systematic review[J]. Clin Oral Implants Res, 2012,23(3):263-273. |
| [14] | Ge J, Yang C, Zheng JW . Autogenous bone grafting for treatment of osseous defect after impacted mandibular third molar extraction: a randomized controlled trial[J]. Clin Implant Dent Relat Res, 2017,19(3):572-580. |
| [15] | Drosos GI, Kazakos KI, Kouzoumpasis P , et al. Safety and eficacy of commercially available demineralised bone matrix preparations: a critical review of clinical studies[J]. Injury, 2007,38(Suppl 41):S13-21. |
| [16] | Allen BA, Moudi E, Majidi MS , et al. A histologic, histomorphometric, and radiographic comparison between two complexes of CenoBoen/CenoMembrane and Bio-Oss/Bio-Gide in lateral ridge augmentation: a clinical trial[J]. Dent Res J (Isfahan), 2016,13(5):446-453. |
| [17] | Ogihara S, Tarnow DP . Efficacy of enamel matrix derivative with freeze-dried bone allograft or demineralized freeze-dried bone allograft in intrabony defects: a randomized trial[J]. J Periodontol, 2014,85(10):1351-1360. |
| [18] | Sammartino G, Tia M, Bucci T , et al. Prevention of mandibular third molar extraction-associated periodontal defects: a comparative study[J]. J Periodontol, 2009,80(3):389-396. |
| [19] | Miron RL, Sculean A, Cochran DL , et al. Twenty years of enamel matrix derivative: the past, the present and the future[J]. J Clin Periodontol, 2016,43(8):668-683. |
| [20] | Ho KN, Salamanca E, Chang KC , et al. A novel HA/β-TCP-collagen composite enhanced new bone formation for dental extraction socket preservation in beagle dogs[J]. Materials (Basel), 2016,9(3):191. |
| [21] | Arenaz-Búa J, Luaces-Rey R, Sironvalle-Soliva S , et al. A comparative study of platelet-rich plasma, hydroxyapatite, demineralized bone matrix and autologous bone to promote bone regeneration after mandibular impacted third molar extraction[J]. Med Oral Patol Oral Cir Bucal, 2010,15(3):e483-489. |
| [22] | Aloy-Prósper A, García-Mira B, Larrazabal-Morón C , et al. Distal probing depth and attachment level of lower second molars following surgical extraction of lower third molars: a literature review[J]. Med Oral Patol Oral Cir Bucal, 2010,15(5):e755-759. |
| [23] | Aimetti M, Romano F . Use of resorbable membranes in periodontal defects treatment after extraction of impacted mandibular third molars[J]. Minerva Stomatol, 2007,56(10):497-508. |
| [24] | Sammartino G, Tia M, Gentile E . Platelet-rich plasma and resorbable membrane for prevention of periodontal defects after deeply impacted lower third molar extraction[J]. J Oral Maxillofac Surg, 2009,67(11):2369-2373. |
| [25] | Moghe S, Saini N, Moghe A . Platelet-rich plasma in periodontal defect treatment after extraction of impacted mandibular third molars. Natl J Maxillofac Surg, 2012,3(2):139-143. |
| [26] | Montero J, Mazzaglia G . Effect of removing an impacted mandibular third molar on the periodontal status of the mandibular second molar[J]. J Oral Maxillofac Surg, 2011,69(11):2691-2697. |
| [27] | Kugelberg CF, Ahlström U, Ericson S , et al. The influence of anatomical, pathophysiological and other factors on periodontal healing after impacted lower third molar surgery a multiple regression analysis[J]. J Clin Periodontol, 1991,18(1):37-43. |
| [28] | Richardson DT, Dodson TB . Risk of periodontal defects after third molar surgery: an exercise in evidence-based clinical decision-making[J]. Oral Surg Oral Med Oral Path Oral Radiol Endod, 2005,100(2):133-137. |
| [29] | Osborne WH, Snyder AJ, Tempel TR . Attachment levels and crevicular depths at the distal of mandibular second molars following removal of adjacent third molars[J]. J Periodontol, 1982,53(2):93-95. |
| [30] | Chen YW, Lee CT, Chuang SK . Effect of flap design on periodontal healing after impacted third molar extraction: a systematic review and meta-analysis[J]. Int J Oral Maxillofac Surg, 2017,46(3):363-372. |
| [31] | Korkmaz YT, Mollaoglu N, Ozmeriç N . Does laterally rotated flap design influence the short-term periodontal status of second molars and postoperative discomfort after partially impacted third molar surgery[J]. J Oral Maxillofac Surg, 2015,73(6):1031-1041. |
| [32] | Kilinc A, Ataol M . How effective is collagen resorbable membrane placement after partially impacted mandibular third molar surgery on postoperative morbidity? A prospective randomized comparative study[J]. BMC Oral Health, 2017,17(1):126. |
| [1] | Sui LI,Wenjie MA,Shimin WANG,Qian DING,Yao SUN,Lei ZHANG. Trueness of different digital design methods for incisal guidance of maxillary anterior implant-supported single crowns [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 81-87. |
| [2] | Xiaoqiang LIU,Yin ZHOU. Risk factors of perioperative hypertension in dental implant surgeries with bone augmentation [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 93-98. |
| [3] | Deng-hui DUAN,Hom-Lay WANG,En-bo WANG. Role of collagen membrane in modified guided bone regeneration surgery using buccal punch flap approach: A retrospective and radiographical cohort study [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1097-1104. |
| [4] | Min ZHEN,Huan-xin MENG,Wen-jie HU,Deng-cheng WU,Yi-ping WEI. Healing of the dento-gingival junction following modified crown lengthening procedure in beagle dogs [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 927-935. |
| [5] | JIANG You-sheng,FENG Lin,GAO Xue-jun. Influence of base materials on stress distribution in endodontically treated maxillary premolars restored with endocrowns [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 764-769. |
| [6] | HUANG Li-dong,GONG Wei-yu,DONG Yan-mei. Effects of bioactive glass on proliferation, differentiation and angiogenesis of human umbilical vein endothelial cells [J]. Journal of Peking University (Health Sciences), 2021, 53(2): 371-377. |
| [7] | WANG Si-wen,YOU Peng-yue,LIU Yu-hua,WANG Xin-zhi,TANG Lin,WANG Mei. Efficacy of two barrier membranes and deproteinized bovine bone mineral on bone regeneration in extraction sockets: A microcomputed tomographic study in dogs [J]. Journal of Peking University (Health Sciences), 2021, 53(2): 364-370. |
| [8] | JIANG Nan,BAO Xu-dong,YUE Lin. Influence of trueness for local finish lines of a full crown preparation on that of complete finish line [J]. Journal of Peking University (Health Sciences), 2021, 53(1): 102-108. |
| [9] | . [J]. Journal of Peking University (Health Sciences), 2020, 52(2): 395-403. |
| [10] | Qian WANG,Dan LI,Zhi-hui TANG. Sinus floor elevation and simultaneous dental implantation: A long term retrospective study of sinus bone gain [J]. Journal of Peking University(Health Sciences), 2019, 51(5): 925-930. |
| [11] | Wei QI,Jian-nan LI,Jing-ren ZHAO,Hai-xia XING,Jie PAN. Effect of triangular flap design and healing procedure on the sequelae after extraction of impacted lower third molars [J]. Journal of Peking University(Health Sciences), 2019, 51(5): 949-953. |
| [12] | Li-ping ZHAO,Wen-jie HU,Tao XU,Ya-lin ZHAN,Yi-ping WEI,Min ZHEN,Cui WANG. Two procedures for ridge preservation of molar extraction sites affected by severe bone defect due to advanced periodontitis [J]. Journal of Peking University(Health Sciences), 2019, 51(3): 579-585. |
| [13] | Jing WANG,Jun-peng CHEN,Yang WANG,Xiang-liang XU,Chuan-bin GUO. Application of digital mandibular movement record and masticatory muscle electromyography in the evaluation of stomatognathic function in patients with mandibular tumor [J]. Journal of Peking University(Health Sciences), 2019, 51(3): 571-578. |
| [14] | Zhi-yong△ ZHANG,Tian MENG,Quan CHEN,Wen-shu LIU,Yu-huan CHEN. Retrospective analysis of early dental implant failure [J]. Journal of Peking University(Health Sciences), 2018, 50(6): 1088-1091. |
| [15] | WU Min-jie, ZOU Li-dong, LIANG Feng. Clinical observation on soft and hard tissue changes of immediate implantation and immediate reconstruction in anterior region after loading 3 years [J]. Journal of Peking University(Health Sciences), 2018, 50(4): 694-699. |
|
||