Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (1): 109-119. doi: 10.19723/j.issn.1671-167X.2021.01.017
Previous Articles Next Articles
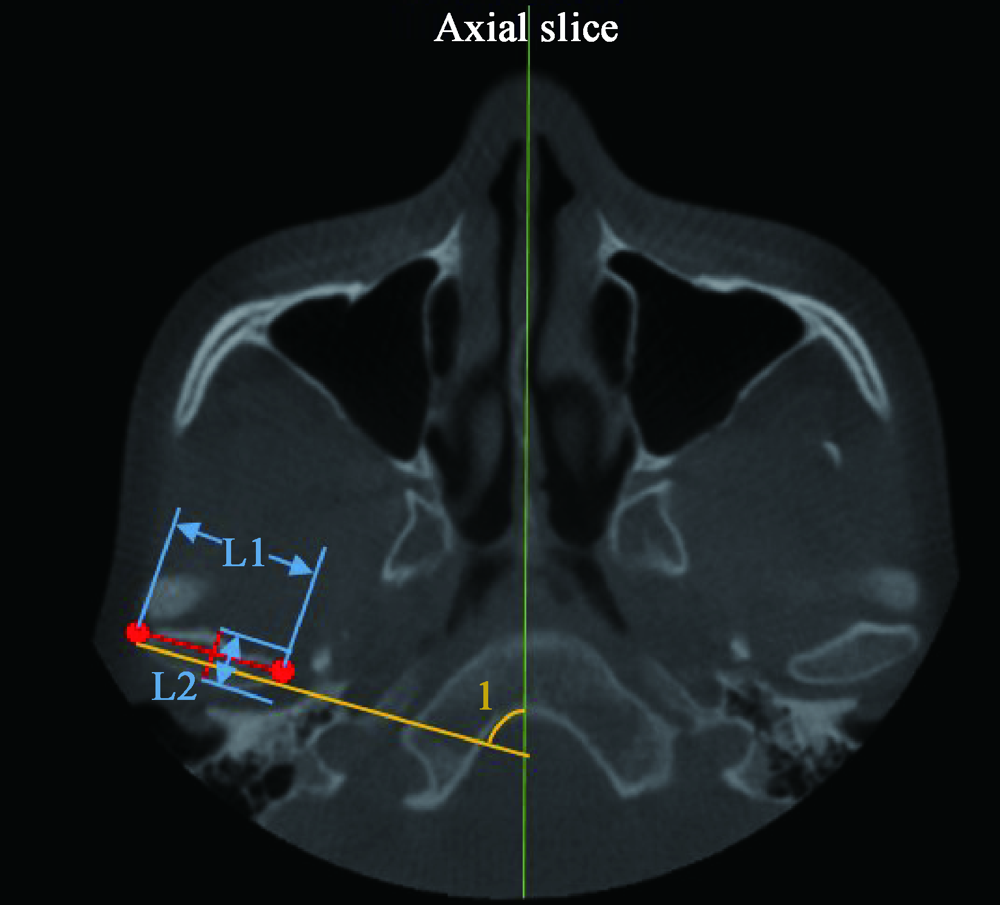
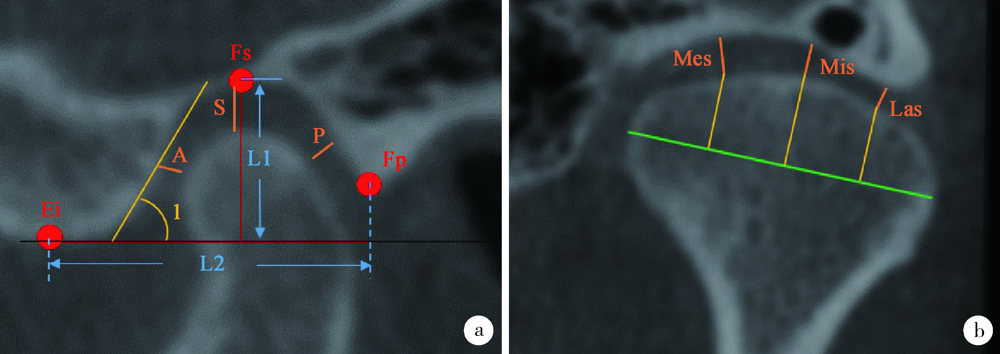
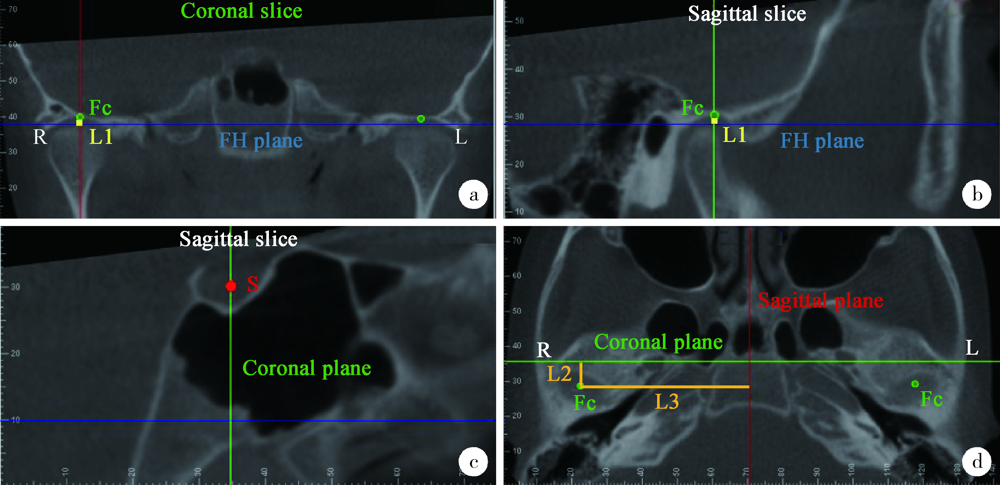
Cone-beam CT evaluation of temporomandibular joint in skeletal class Ⅱ female adolescents with different vertical patterns
ZHOU Jing,LIU Yi( )
)
- Department of Orthodontics, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
CLC Number:
- R783.5





| [1] |
Bjork A. Facial growth in man, studied with the aid of metallic implants[J]. Acta Odontol Scand, 1955,13(1):9-34.
doi: 10.3109/00016355509028170 pmid: 14398173 |
| [2] |
Copray JC, Dibbets JM, Kantomaa T. The role of condylar cartilage in the development of the temporomandibular joint[J]. Angle Orthod, 1988,58(4):369-380.
pmid: 3061315 |
| [3] |
Weinberg LA. Correlation of temporomandibular dysfunction with radiographic findings[J]. J Prosthet Dent, 1972,28(5):519-539.
doi: 10.1016/0022-3913(72)90064-9 pmid: 4507574 |
| [4] |
Ahn SJ, Lee SJ, Kim TW. Orthodontic effects on dentofacial morphology in women with bilateral TMJ disk displacement[J]. Angle Orthod, 2007,77(2):288-295.
pmid: 17319764 |
| [5] |
McNamara JA Jr. Components of class Ⅱ malocclusion in children 8-10 years of age[J]. Angle Orthod, 1981,51(3):177-202.
doi: 10.1043/0003-3219(1981)051<0177:COCIMI>2.0.CO;2 pmid: 7023290 |
| [6] |
Simmons 3rd HC, Oxford DE, Hill MD. The prevalence of skeletal Class Ⅱ patients found in a consecutive population presenting for TMD treatment compared to the national average[J]. J Tenn Dent Assoc, 2008,88(4):16-18.
pmid: 19248341 |
| [7] | Lin M, Xu Y, Wu H, et al. Comparative cone-beam computed tomography evaluation of temporomandibular joint position and morphology in female patients with skeletal class Ⅱ malocclusion[J]. J Int Med Res, 2019,48(2):0300060519892388. |
| [8] |
Hasebe A, Yamaguchi T, Nakawaki T, et al. Comparison of condylar size among different anteroposterior and vertical skeletal patterns using cone-beam computed tomography[J]. Angle Orthod, 2019,89(2):306-311.
doi: 10.2319/032518-229.1 pmid: 30475648 |
| [9] |
Ma Q, Bimal P, Mei L, et al. Temporomandibular condylar morphology in diverse maxillary-mandibular skeletal patterns: A 3-dimensional cone-beam computed tomography study[J]. J Am Dent Assoc, 2018,149(7):589-598.
doi: 10.1016/j.adaj.2018.02.016 pmid: 29655707 |
| [10] |
Pullinger A, Hollender L. Variation in condyle-fossa relationships according to different methods of evaluation in tomograms[J]. Oral Surg Oral Med Oral Pathol, 1986,62(6):719-727.
doi: 10.1016/0030-4220(86)90270-7 pmid: 3467295 |
| [11] | Ocak M, Sargon MF, Orhan K, et al. Evaluation of the anatomical measurements of the temporomandibular joint by cone-beam computed tomography[J]. Folia Morphol, 2019,78(1):174-181. |
| [12] |
Tsiklakis K, Syriopoulos K, Stamatakis HC. Radiographic examination of the temporomandibular joint using cone beam computed tomography[J]. Dentomaxillofac Radiol, 2004,33(3):196-201.
doi: 10.1259/dmfr/27403192 pmid: 15371321 |
| [13] |
Firetto MC, Abbinante A, Barbato E, et al. National guidelines for dental diagnostic imaging in the developmental age[J]. Radiol Med, 2019,124(9):887-916.
doi: 10.1007/s11547-019-01038-4 pmid: 31055724 |
| [14] | Bjork A. Variations in the growth pattern of the human mandible: Longitudinal radiographic study by the implant method[J]. J Dent Res, 1963,42(1):400-411. |
| [15] |
Lobo F, Tolentino ES, Iwaki LCV, et al. Imaginology tridimensional study of temporomandibular joint osseous components according to sagittal skeletal relationship, sex, and age[J]. J Craniofac Surg, 2019,30(5):1462-1465.
doi: 10.1097/SCS.0000000000005467 pmid: 31299744 |
| [16] |
Al-koshab M, Nambiar P, John J. Assessment of condyle and glenoid fossa morphology using CBCT in South-East Asians[J]. PLoS One, 2015,10(3):e0121682.
doi: 10.1371/journal.pone.0121682 pmid: 25803868 |
| [17] |
Coombs MC, She X, Brown T R, et al. Temporomandibular joint condyle-disc morphometric sexual dimorphisms independent of skull scaling[J]. J Oral Maxillofac Surg, 2019,77(11):2245-2257.
doi: 10.1016/j.joms.2019.04.022 pmid: 31125537 |
| [18] |
Weinberg LA. Role of condylar position in TMJ dysfunction-pain syndrome[J]. J Prosthet Dent, 1979,41(6):636-643.
doi: 10.1016/0022-3913(79)90062-3 pmid: 286056 |
| [19] | 葛胜将. 不同骨性错牙合患者髁突形态及位置的CBCT研究[D]. 青岛: 青岛大学, 2015. |
| [20] | 韩晓利. 成年女性骨性Ⅱ错牙合不同垂直骨面型患者TMJ骨性结构特征的CBCT研究[D]. 天津: 天津医科大学, 2017. |
| [21] | 崔燕, 唐天琪, 刘琳. 不同矢状骨面型患者颞下颌关节形态特征锥形束CT研究[J]. 中国实用口腔科杂志, 2016,9(6):348-353. |
| [22] |
Saccucci M, Polimeni A, Festa F, et al. Do skeletal cephalometric characteristics correlate with condylar volume, surface and shape? A 3D analysis[J]. Head Face Med, 2012,8:15.
doi: 10.1186/1746-160X-8-15 pmid: 22587445 |
| [23] |
Katayama K, Yamaguchi T, Sugiura M, et al. Evaluation of mandibular volume using cone-beam computed tomography and correlation with cephalometric values[J]. Angle Orthod, 2014,84(2):337-342.
doi: 10.2319/012913-87.1 pmid: 23985034 |
| [24] |
Paknahad M, Shahidi S, Abbaszade H. Correlation between condylar position and different sagittal skeletal facial types[J]. J Orofac Orthop, 2016,77(5):350-356.
doi: 10.1007/s00056-016-0039-z pmid: 27357584 |
| [25] |
Nielsen IL. Vertical malocclusions: etiology, development, diagnosis and some aspects of treatment[J]. Angle Orthod, 1991,61(4):247-260.
doi: 10.1043/0003-3219(1991)061<0247:VMEDDA>2.0.CO;2 pmid: 1763835 |
| [26] |
Droel R, Isaacson RJ. Some relationships between the glenoid fossa position and various skeletal discrepancies[J]. Am J Orthod, 1972,61(1):64-78.
doi: 10.1016/0002-9416(72)90177-7 pmid: 4500188 |
| [27] |
Costa EDD, Peyneau PD, Roque-Torres GD, et al. The relationship of articular eminence and mandibular fossa morphology to facial profile and gender determined by cone beam computed tomography[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2019,128(6):660-666.
doi: 10.1016/j.oooo.2019.07.007 pmid: 31494114 |
| [28] |
Kurusu A, Horiuchi M, Soma K. Relationship between occlusal force and mandibular condyle morphology. Evaluated by limited cone-beam computed tomography[J]. Angle Orthod, 2009,79(6):1063-1069.
doi: 10.2319/120908-620R.1 pmid: 19852595 |
| [29] |
Burke G, Major P, Glover K, et al. Correlations between condylar characteristics and facial morphology in Class Ⅱ preadolescent patients[J]. Am J Orthod Dentofacial Orthop, 1998,114(3):328-336.
doi: 10.1016/s0889-5406(98)70216-1 pmid: 9743139 |
| [30] | 李晨. 不同垂直骨面型骨性Ⅱ类成年女性颞下颌关节骨性结构的三维分析[D]. 西安: 第四军医大学, 2016. |
| [31] |
Goymen M, Gulec A. Effects of the vertical malocclusion types on the dimension of the mandibular condyle[J]. Turk J Orthod, 2017,30(4):106-109.
doi: 10.5152/TurkJOrthod.2017.17029 pmid: 30112501 |
| [32] | 车蓓, 张昊, 钱才梅, 等. 不同垂直骨面型安氏Ⅱ类1分类错牙合患者颞下颌关节三维形态结构的比较[J]. 中华口腔医学杂志, 2014,49(7):399-402. |
| [33] |
Celik S, Celikoglu M, Buyuk SK, et al. Mandibular vertical asymmetry in adult orthodontic patients with different vertical growth patterns: A cone beam computed tomography study[J]. Angle Orthod, 2016,86(2):271-277.
doi: 10.2319/030515-135.1 pmid: 26065465 |
| [34] |
Kikuchi K, Takeuchi S, Tanaka E, et al. Association between condylar position, joint morphology and craniofacial morphology in orthodontic patients without temporomandibular joint disorders[J]. J Oral Rehabil, 2003,30(11):1070-1075.
doi: 10.1046/j.1365-2842.2003.01194.x pmid: 14641670 |
| [35] |
Paknahad M, Shahidi S. Association between condylar position and vertical skeletal craniofacial morphology: a cone beam computed tomography study[J]. Int Orthod, 2017,15(4):740-751.
doi: 10.1016/j.ortho.2017.09.008 pmid: 29111128 |
| [36] |
Park IY, Kim JH, Park YH. Three-dimensional cone-beam computed tomography based comparison of condylar position and morphology according to the vertical skeletal pattern[J]. Korean J Orthod, 2015,45(2):66-73.
doi: 10.4041/kjod.2015.45.2.66 pmid: 25798412 |
| [1] | Shishi BO,Chengzhi GAO. Tooth segmentation and identification on cone-beam computed tomography with convolutional neural network based on spatial embedding information [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 735-740. |
| [2] | Hejun SHEN,Chongyan SHI,Qing ZHENG,Yu HUANG,Tao JING. Investigation on the current situation and influencing factors of sitting time and health literacy among high school students in China [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 239-246. |
| [3] | Hongguang LI,Weihua HAN,Xun WU,Jiling FENG,Gang LI,Juanhong MENG. Preliminarily study of arthrocentesis combined with liquid phase concentrated growth factor injection in the treatment of unilateral temporomandibular joint osteoarthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 338-344. |
| [4] | Bochun MAO,Yajing TIAN,Xuedong WANG,Jing LI,Yanheng ZHOU. Soft and hard tissue changes of hyperdivergent class Ⅱ patients before and after orthodontic extraction treatment [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 111-119. |
| [5] | Xiaotong LING,Liuyang QU,Danni ZHENG,Jing YANG,Xuebing YAN,Denggao LIU,Yan GAO. Three-dimensional radiographic features of calcifying odontogenic cyst and calcifying epithelial odontogenic tumor [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 131-137. |
| [6] | Deng-hui DUAN,Hom-Lay WANG,En-bo WANG. Role of collagen membrane in modified guided bone regeneration surgery using buccal punch flap approach: A retrospective and radiographical cohort study [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1097-1104. |
| [7] | Meng-jie CUI,Qi MA,Man-man CHEN,Tao MA,Xin-xin WANG,Jie-yu LIU,Yi ZHANG,Li CHEN,Jia-nuo JIANG,Wen YUAN,Tong-jun GUO,Yan-hui DONG,Jun MA,Yi XING. Association between different growth patterns and metabolic syndrome in children and adolescents aged 7 to 17 years [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 415-420. |
| [8] | Jia-jia DANG,Shan CAI,Pan-liang ZHONG,Ya-qi WANG,Yun-fei LIU,Di SHI,Zi-yue CHEN,Yi-hang ZHANG,Pei-jin HU,Jing LI,Jun MA,Yi SONG. Association of outdoor artificial light at night exposure with overweight and obesity among children and adolescents aged 9 to 18 years in China [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 421-428. |
| [9] | Dan-feng ZHENG,Jun-yu LI,Jia-xi LI,Ying-shuang ZHANG,Yan-feng ZHONG,Miao YU. Pathologic features of paraspinal muscle biopsies in patients with adolescent idiopathic scoliosis [J]. Journal of Peking University (Health Sciences), 2023, 55(2): 283-291. |
| [10] | Jin-hua ZHANG,Jie PAN,Zhi-peng SUN,Xiao WANG. Effect of various intracanal materials on the diagnostic accuracy of cone-beam computed tomography in vertical root fractures [J]. Journal of Peking University (Health Sciences), 2023, 55(2): 333-338. |
| [11] | Jia-xue YE,Yu-hong LIANG. A prevalence survey of cone-beam computed tomography use among endodontic practitioners [J]. Journal of Peking University (Health Sciences), 2023, 55(1): 114-119. |
| [12] | Meng-qiao PAN,Jian LIU,Li XU,Xiao XU,Jian-xia HOU,Xiao-tong LI,Xiao-xia WANG. A long-term evaluation of periodontal phenotypes before and after the periodontal-orthodontic-orthognathic combined treatment of lower anterior teeth in patients with skeletal Angle class Ⅲ malocclusion [J]. Journal of Peking University (Health Sciences), 2023, 55(1): 52-61. |
| [13] | Yu FU,Xin-nong HU,Sheng-jie CUI,Jie SHI. Decompensation effectiveness and alveolar bone remodeling analysis of mandibular anterior teeth after preoperative orthodontic treatment in high-angle patients with skeletal class Ⅱ malocclusion [J]. Journal of Peking University (Health Sciences), 2023, 55(1): 62-69. |
| [14] | Juan GAO,Hang-miao LV,Hui-min MA,Yi-jiao ZHAO,Xiao-tong LI. Evaluation of root resorption after surgical orthodontic treatment of skeletal Class Ⅲ malocclusion by three-dimensional volumetric measurement with cone-beam CT [J]. Journal of Peking University (Health Sciences), 2022, 54(4): 719-726. |
| [15] | Yun-fei LIU,Jia-jia DANG,Pan-liang ZHONG,Ning MA,Di SHI,Yi SONG. Injury mortality among Chinese aged 5 to 24 years from 1990 to 2019 [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 498-504. |
|
||