Journal of Peking University(Health Sciences) ›› 2019, Vol. 51 ›› Issue (5): 913-918. doi: 10.19723/j.issn.1671-167X.2019.05.020
Previous Articles Next Articles
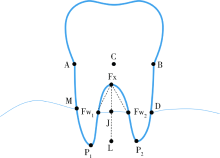
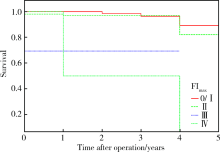
Tooth loss and multivariable analysis after 5-year non-surgical periodontal treatment on molars with furcation involvement
Shu-wen SHI1,Yang MENG2,Jian JIAO1,Wen-jing LI1,Huan-xin MENG1,△( ),Qing-xian LUAN1,Wan-chun WANG2
),Qing-xian LUAN1,Wan-chun WANG2
- 1. Department of Periodontology, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
2. Department of Periodontology, Qingdao Stomatological Hospital, Qingdao 266001, Shandong, China
CLC Number:
- R781.42


| [1] | 孟焕新 . 临床牙周病学[M]. 2版. 北京: 北京大学医学出版社, 2014: 216-219. |
| [2] | 孟洋, 王万春, 栾庆先 . 根分叉病变发生、发展与治疗研究进展[J]. 中国实用口腔医学杂志, 2016,4(9):237-242. |
| [3] | Grover V, Malhotra R, Kapoor A , et al. Correlation of the interdental and the interradicular bone loss: A radiovisuographic analysis[J]. J Indian Soc Periodontol, 2014,18(4):482-487. |
| [4] | Dannewitz B, Krieger JK, Hüsing J , et al. Loss of molars in periodontally treated patients: A retrospective analysis five years or more after active periodontal treatment[J]. J Clin Periodontol, 2006,33(1):53-61. |
| [5] | Do Vale HF, Del Peloso Ribeiro E, Bittencourt S, et al. Radiographic characteristics of furcation involvements in mandibular molars as prognostic indicators of healing after nonsurgical periodontal therapy[J]. J Am Dent Assoc, 2009,140(4):434-440. |
| [6] | Mazza JE, Newman MG, Sims TN . Clinical and antimicrobial effect of stannous fluoride on periodontitis[J]. J Clin Periodontol, 1981,8(3):203-212. |
| [7] | Jiao J, Shi D, Cao ZQ , et al. Effectiveness of non-surgical periodontal therapy in a large Chinese population with chronic periodontitis[J]. J Clin Periodontol, 2017,44(1):42-50. |
| [8] | Hou GL, Hung CC, Tsai CC , et al. Topographic study of root trunk type on Chinese molars with Class Ⅲ furcation involvements: Molar type and furcation site[J]. Int J Periodontics Restorative Dent, 2005,25(2):173-179. |
| [9] | Bowers GM, Schallhorn RG, McClain PK, et al. Factors influen-cing the outcome of regenerative therapy in mandibular class Ⅱ furcations: Part Ⅰ[J]. J Periodontol, 2003,74(9):1255-1268. |
| [10] | James JR, Arun KV, Talwar A , et al. Mathematical analysis of furcation angle in extracted mandibular molars[J]. J Indian Soc Periodontol, 2013,17(1):68-71. |
| [11] | Faggion CM Jr, Petersilka G, Lange DE , et al. Prognostic model for tooth survival in patients treated for periodontitis[J]. J Clin Periodontol, 2007,34(3):226-231. |
| [12] | Checchi L, Montevecchi M, Gatto MR , et al. Retrospective study of tooth loss in 92 treated periodontal patients[J]. J Clin Perio-dontol, 2002,29(7):651-656. |
| [13] | Graetz C, Schützhold S, Plaumann A , et al. Prognostic factors for the loss of molars: An 18-years retrospective cohort study[J]. J Clin Periodontol, 2015,42(10):943-950. |
| [14] | Onabolu O, Donos N, Tu YK , et al. Periodontal progression based on radiographic records: An observational study in chronic and aggressive periodontitis[J]. J Dent, 2015,43(6):673-682. |
| [15] | 沈潇, 施捷, 徐莉 , 等. 伴错牙合畸形的侵袭性牙周炎患者牙周-正畸联合治疗的临床评价[J]. 北京大学学报(医学版), 2017,49(1):60-66. |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Fan SHU, Liyuan GE, Hanzhang DENG, Haoming YIN, Junyong OU, Shaohui DENG, Yichang HAO, Min LU, Zhanyi ZHANG, Peichen DUAN, Shudong ZHANG. Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 631-640. |
| [3] | Lingfu ZHANG, Ming CHEN, Xiaoyu ZHAO, Gang WANG, Long CUI, Xiaofeng LING, Lixin WANG, Zhi XU, Limei GUO, Chunsheng HOU. Gross classification of gallbladder cancer with primary lesion limited to the gallbladder wall and its correlation with prognosis and precancerous lesions [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 184-189. |
| [4] | Boda GUO, Min LU, Guoliang WANG, Hongxian ZHANG, Lei LIU, Xiaofei HOU, Lei ZHAO, Xiaojun TIAN, Shudong ZHANG. Clinicopathological and prognostic differences between clear cell and non-clear cell renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 644-649. |
| [5] | Zhenying BAO, Yajie WANG. Application of combined detection of inflammatory indexes and cytokines in chronic periodontitis [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 772-778. |
| [6] | Weihao LI, Jing LI, Xuemin ZHANG, Wei LI, Qingle LI, Xiaoming ZHANG. Effect of intraoperative blood salvage autotransfusion on the prognosis of patients after carotid body tumor resection [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 272-276. |
| [7] | Lijuan MA, Yonghui TENG, Yong WANG, Yijiao ZHAO, Xinyue ZHANG, Qingzhao QIN, Dong YIN. Three-dimensional finite element analysis of digital wire loop space maintainers for missing deciduous teeth [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 376-383. |
| [8] | Yaqing MAO, Zhen CHEN, Yao YU, Wenbo ZHANG, Yang LIU, Xin PENG. Impact of type 2 diabetes mellitus on the prognosis of patients with oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1089-1096. |
| [9] | Junyong OU,Kunming NI,Lulin MA,Guoliang WANG,Ye YAN,Bin YANG,Gengwu LI,Haodong SONG,Min LU,Jianfei YE,Shudong ZHANG. Prognostic factors of patients with muscle invasive bladder cancer with intermediate-to-high risk prostate cancer [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 582-588. |
| [10] | Shuai LIU,Lei LIU,Zhuo LIU,Fan ZHANG,Lulin MA,Xiaojun TIAN,Xiaofei HOU,Guoliang WANG,Lei ZHAO,Shudong ZHANG. Clinical treatment and prognosis of adrenocortical carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 624-630. |
| [11] | Le YU,Shaohui DENG,Fan ZHANG,Ye YAN,Jianfei YE,Shudong ZHANG. Clinicopathological characteristics and prognosis of multilocular cystic renal neoplasm of low malignant potential [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 661-666. |
| [12] | Zezhen ZHOU,Shaohui DENG,Ye YAN,Fan ZHANG,Yichang HAO,Liyuan GE,Hongxian ZHANG,Guoliang WANG,Shudong ZHANG. Predicting the 3-year tumor-specific survival in patients with T3a non-metastatic renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 673-679. |
| [13] | Yangyi FANG,Qiang LI,Zhigao HUANG,Min LU,Kai HONG,Shudong ZHANG. Well-differentiated papillary mesothelial tumour of the tunica vaginalis: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 741-744. |
| [14] | Yuanyuan ZENG,Yun XIE,Daonan CHEN,Ruilan WANG. Related factors of euthyroid sick syndrome in patients with sepsis [J]. Journal of Peking University (Health Sciences), 2024, 56(3): 526-532. |
| [15] | Jian-bin LI,Meng-na LYU,Qiang CHI,Yi-lin PENG,Peng-cheng LIU,Rui WU. Early prediction of severe COVID-19 in patients with Sjögren’s syndrome [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1007-1012. |
|
||