Journal of Peking University(Health Sciences) ›› 2020, Vol. 52 ›› Issue (1): 30-34. doi: 10.19723/j.issn.1671-167X.2020.01.005
Previous Articles Next Articles
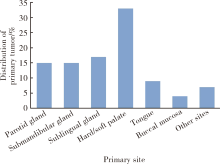
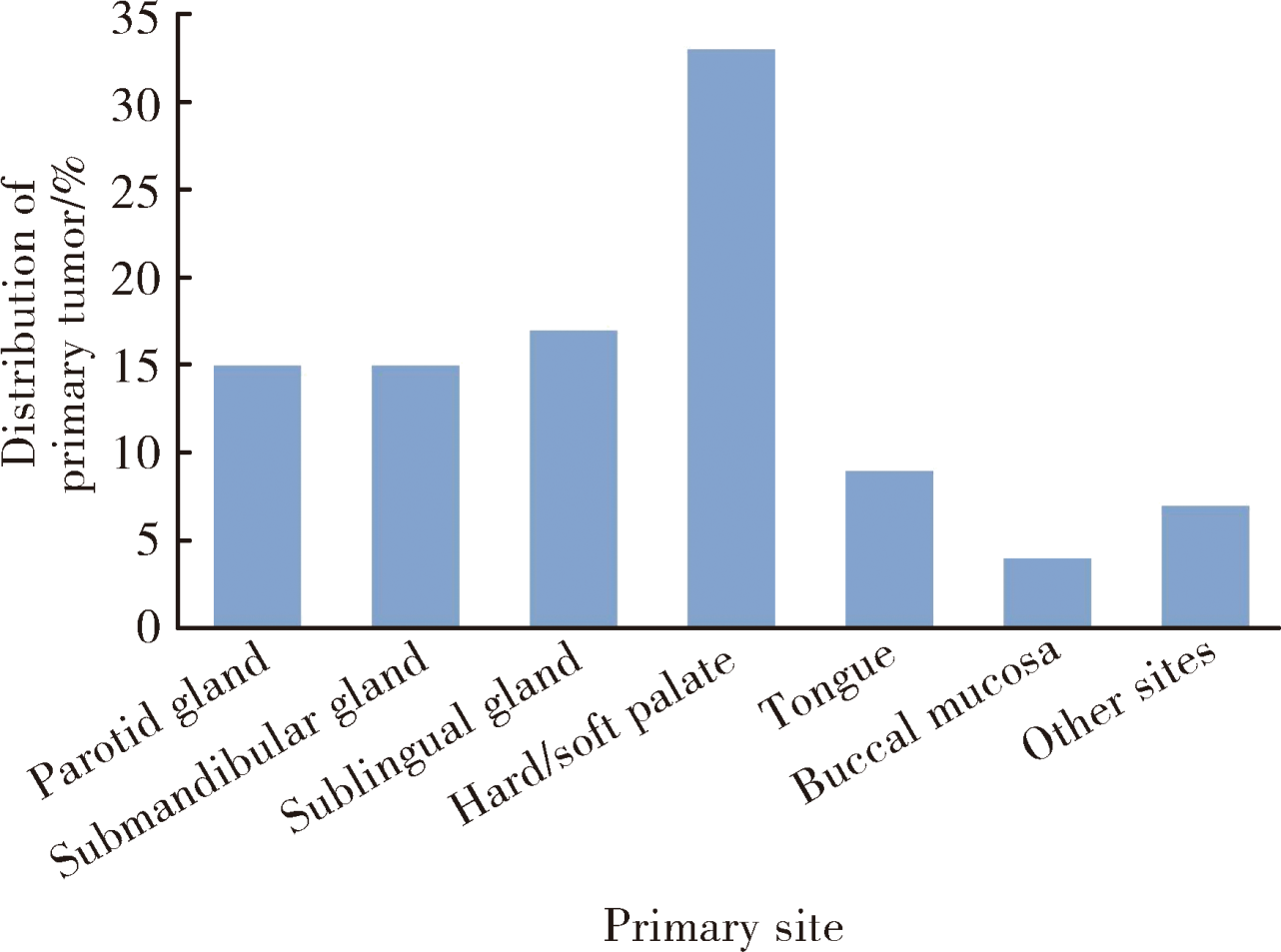
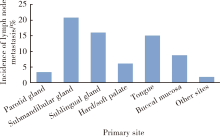
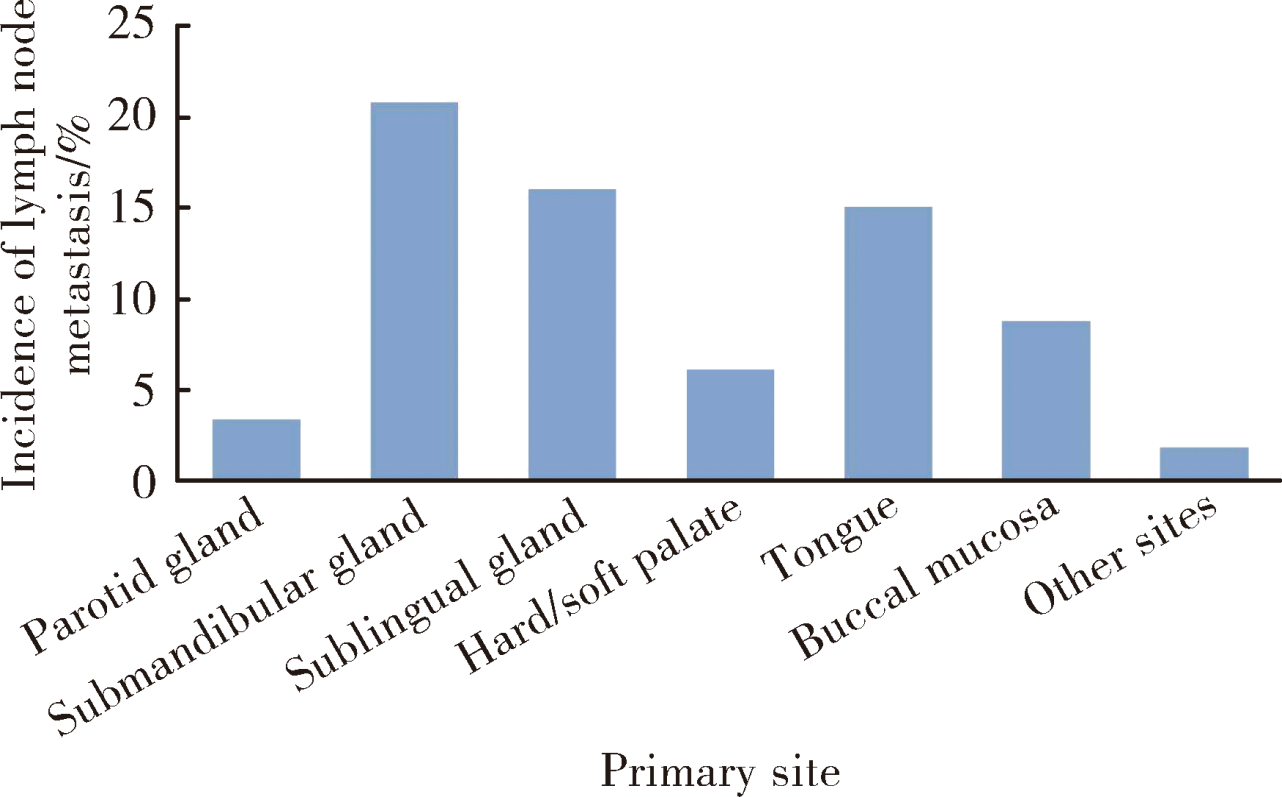
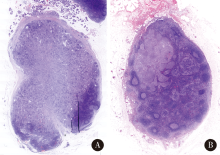
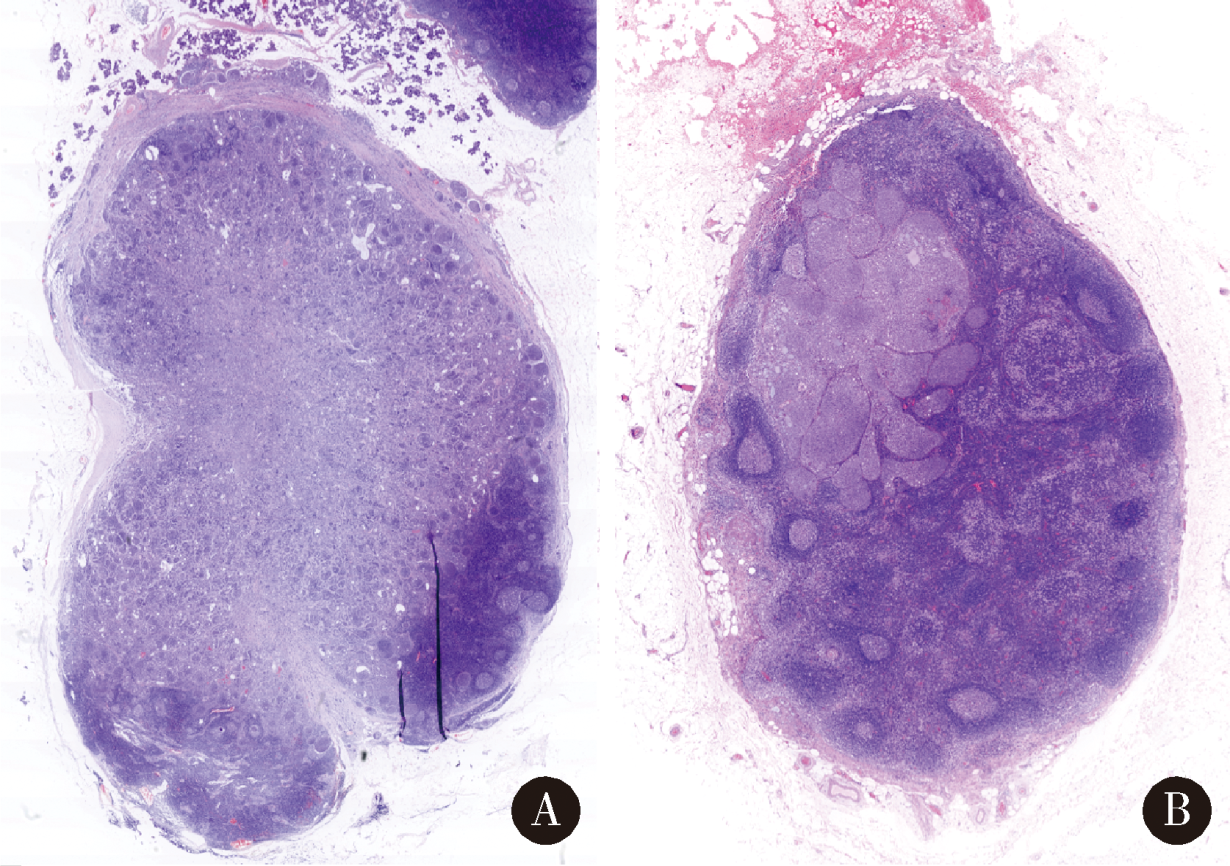
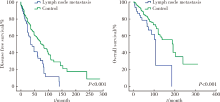
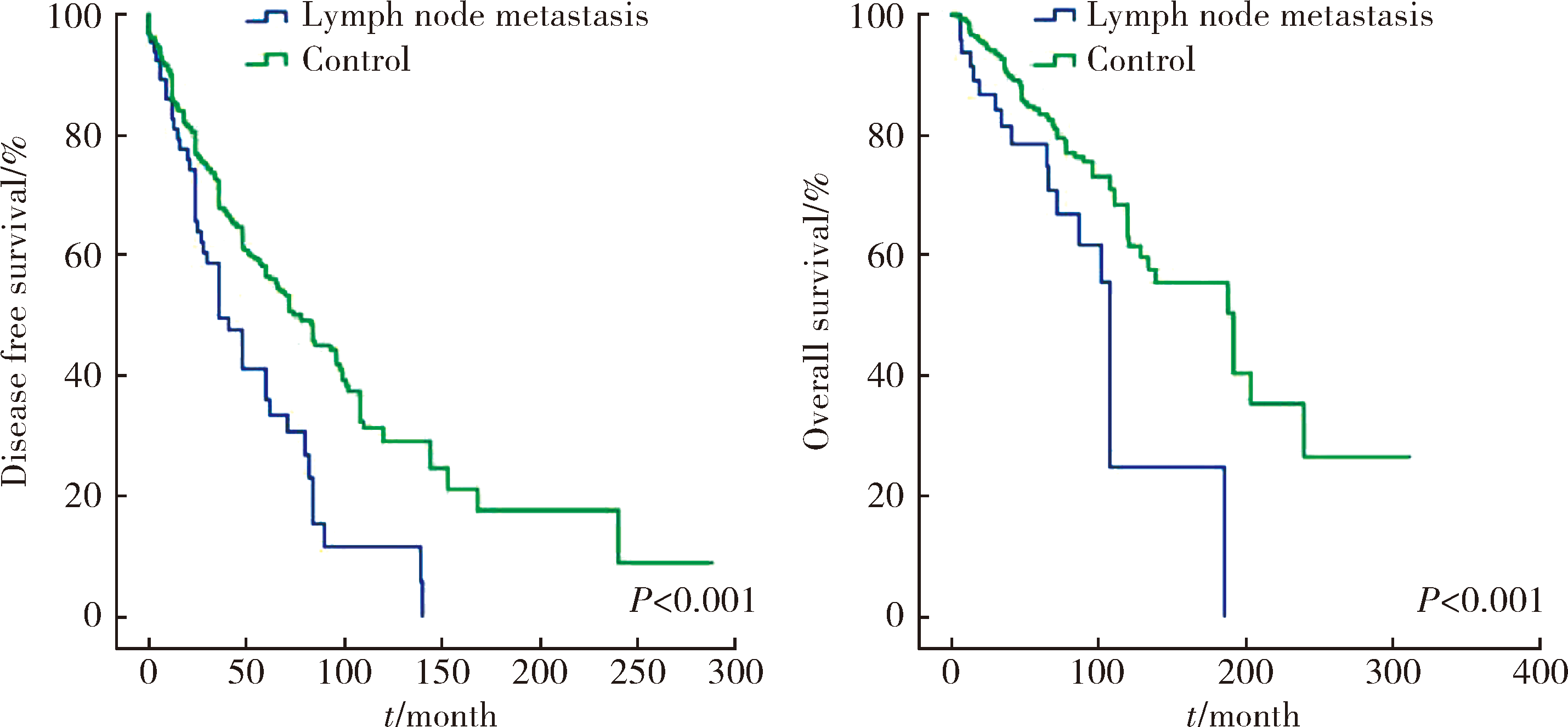
Cervical lymph node metastasis in adenoid cystic carcinoma of the salivary glands: A clinicopathologic study
Ye ZHANG,Ni ZHANG,Xiao-xiao LIU,Chuan-xiang ZHOU( )
)
- Department of Oral Pathology, Peking University School and Hospital of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Laboratory for Digital and Material Technology of Stomatology & Beijing Key Laboratory of Digital Stomatology, Beijing 100081, China
CLC Number:
- R739.87


| [1] | Tian Z, Li L, Wang L , et al. Salivary gland neoplasms in oral and maxillofacial regions: A 23-year retrospective study of 6 982 cases in an eastern Chinese population[J]. Int J Oral Maxillofac Surg, 2010,39(3):235-242. |
| [2] | Gao M, Hao Y, Huang MX , et al. Clinicopathological study of distant metastases of salivary adenoid cystic carcinoma[J]. Int J Oral Maxillofac Surg, 2013,42(8):923-928. |
| [3] | Shen C, Xu T, Huang C , et al. Treatment outcomes and prognostic features in adenoid cystic carcinoma originated from the head and neck[J]. Oral Oncol, 2012,48(5):445-449. |
| [4] | Lloyd S, Yu JB, Wilson LD , et al. Determinants and patterns of survival in adenoid cystic carcinoma of the head and neck, including an analysis of adjuvant radiation therapy[J]. Am J Clin Oncol, 2011,34(1):76-81. |
| [5] | Bhayani MK, Yener M, El-Naggar A , et al. Prognosis and risk factors for early-stage adenoid cystic carcinoma of the major salivary glands[J]. Cancer, 2012,118(11):2872-2878. |
| [6] | Armstrong JG, Harrison LB, Thaler HT , et al. The indications for elective treatment of the neck in cancer of the major salivary glands[J]. Cancer, 1992,69(3):615-619. |
| [7] | Suárez C, Barnes L, Silver CE , et al. Cervical lymph node metastasis in adenoid cystic carcinoma of oral cavity and oropharynx: A collective international review[J]. Auris Nasus Larynx, 2016,43(5):477-484. |
| [8] | Ardekian L, Kokemueller H, Eckardt A , et al. Adenoid cystic carcinoma of the head and neck: A 20 years experience[J]. Int J Oral Maxillofac Surg, 2004,33(1):25-31. |
| [9] | Bianchi B, Copelli C, Cocchi R , et al. Adenoid cystic carcinoma of intraoral minor salivary glands[J]. Oral Oncol, 2008,44(11):1026-1031. |
| [10] | Coca-Pelaz A, Rodrigo JP, Bradley PJ , et al. Adenoid cystic carcinoma of the head and neck: An update[J]. Oral Oncol, 2015,51(7):652-661. |
| [11] | Zhang M, Xu ZF, Tao Y , et al. Clinical analysis of 25 patients with glossal adenoid cystic carcinoma[J]. Int J Stomt, 2009,36(2):148-151. |
| [12] | Min R, Siyi L, Wenjun Y , et al. Salivary gland adenoid cystic carcinoma with cervical lymph node metastasis: A preliminary study of 62 cases[J]. Int J Oral Maxillofac Surg, 2012,41(8):952-957. |
| [13] | Amit M, Binenbaum Y, Sharma K , et al. Incidence of cervical lymph node metastasis and its association with outcomes in patients with adenoid cystic carcinoma. An international collaborative study[J]. Head Neck, 2015,37(7):1032-1037. |
| [14] | Weinreb I, Lee SY, Kim BH , et al. Nineteen-year oncologic outcomes and the benefit of elective neck dissection in salivary gland adenoid cystic carcinoma[J]. Head Neck, 2014,36(12):1796-1801. |
| [15] | Ali S, Palmer FL, Katabi N , et al. Long-term local control rates of patients with adenoid cystic carcinoma of the head and neck managed by surgery and postoperative radiation[J]. Laryngoscope, 2017,127(10):2265-2269. |
| [16] | Nakada M, Nishizaki K, Akagi H , et al. Oncocytic carcinoma of the submandibular gland: a case report and literature review[J]. J Oral Pathol Med, 1998,27(5):225-228. |
| [17] | Amit M, Na’ara S, Sharma K , et al. Elective neck dissection in patients with head and neck adenoid cystic carcinoma: An international collaborative study[J]. Ann Surg Oncol, 2015,22(4):1353-1359. |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Fan SHU, Liyuan GE, Hanzhang DENG, Haoming YIN, Junyong OU, Shaohui DENG, Yichang HAO, Min LU, Zhanyi ZHANG, Peichen DUAN, Shudong ZHANG. Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 631-640. |
| [3] | Hao FU, Luyan SHEN, Bingyang HUANG, Shaohua MA. Clinical strategies for perioperative management of esophageal squamous cell carcinoma in the immunotherapy era [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 266-271. |
| [4] | Nannan WANG, Dajin YUAN, Yubing ZHU, Lei DING. Development and validation of a multicenter nomogram predicting the risk of liver metastasis after curative resection of colorectal cancer [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 290-300. |
| [5] | Haoming YIN, Zijie WANG, Fan SHU, Zhanyi ZHANG, Hui LIANG, Shudong ZHANG. Expression and significance of the FABP6 long transcript in clear cell renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 393-398. |
| [6] | Jialin LI, Liqiao CHEN, Jiatian TANG, Yan WU, Anqiang WANG. Conversion therapy for hepatoid adenocarcinoma of the stomach: A case report [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 399-404. |
| [7] | Zichen PAN, Kai CHEN, Yukun HOU, Bohan YANG, Jixin ZHANG, Yongsu MA, Xiaodong TIAN, Yinmo YANG. Research progress in clinical pathology and molecular mechanisms of pancreatic adenosquamous carcinoma [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 431-435. |
| [8] | Xin CONG, Jiazeng SU, Liling WU, Chong DING, Wei LI, Guangyan YU. Research progress in diagnosis and treatment of non-tumorous salivary gland diseases [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 1-9. |
| [9] | Xiaolin WANG, Luyao LI, Wen ZHANG, Hongyan WANG. Clinicopathological analysis of mesonephric-like adenocarcinoma in the corpusuteri: A report of 3 cases [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1208-1212. |
| [10] | Weihua HOU, Shujie SONG, Zhongyue SHI, Lu LIU, Mulan JIN. Neuroendocrine carcinoma with significantly vacuolar nucleus at the esophagogastric junction: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 1005-1009. |
| [11] | Shang XIE, Luming WANG, Xinyuan ZHANG, Qiushi FENG, Yangyang XIA, Ziwei DAI, Xiaofeng SHAN, Zhigang CAI. Construction and application of oral squamous cell carcinoma organoid bank [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 847-851. |
| [12] | Shaohai TANG, Baoming YANG, Jiankun LI, Lili ZHAO, Yifan WANG, Shunxiang WANG. HDAC2-mediated H3K27 acetylation promotes the proliferation and migration of hepatocellular carcinoma cells [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 884-894. |
| [13] | Xiaoyong YANG, Fan ZHANG, Lulin MA, Cheng LIU. Clinical characteristics and influencing factors of extraglandular invasion of prostatic ductal adenocarcinoma [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 956-960. |
| [14] | Shenmo LI, Dandan SU, Jiyu LIN, Haodong SONG, Lulin MA, Xiaofei HOU, Guoliang WANG, Hongxian ZHANG, Jianfei YE, Shudong ZHANG. Prognostic analysis of laparoscopic simultaneous radical cystectomy and nephroureterectomy [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 961-966. |
| [15] | Boda GUO, Min LU, Guoliang WANG, Hongxian ZHANG, Lei LIU, Xiaofei HOU, Lei ZHAO, Xiaojun TIAN, Shudong ZHANG. Clinicopathological and prognostic differences between clear cell and non-clear cell renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 644-649. |
|
||