Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (5): 850-856. doi: 10.19723/j.issn.1671-167X.2021.05.007
Previous Articles Next Articles
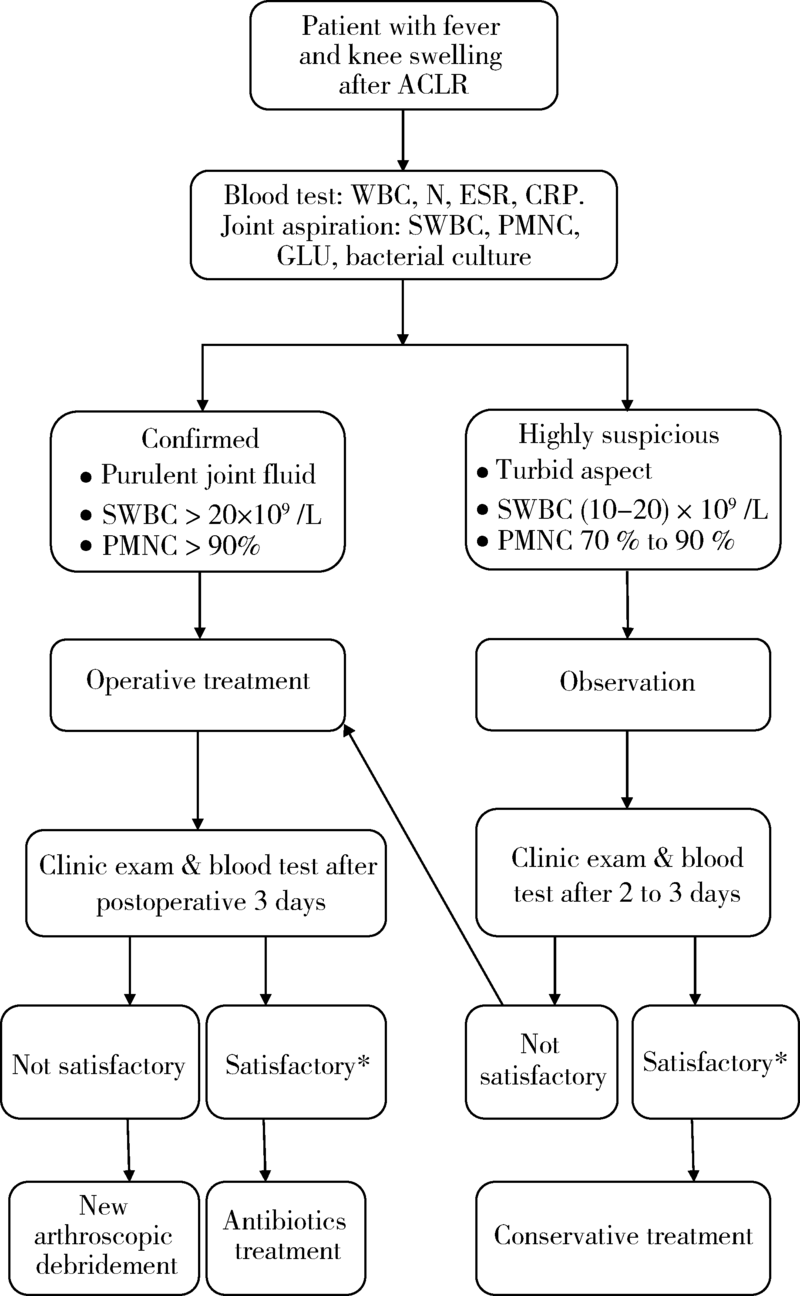
Management algorithm for septic arthritis after anterior cruciate ligament reconstruction
WANG Cheng1,MENG Ling-yu2,CHEN Na-yun1,LI Dai1,WANG Jian-quan1,AO Ying-fang1,△( )
)
- 1. Department of Sports Medicine, Peking University Third Hospital, Institute of Sports Medicine of Peking University, Beijing Key Laboratory of Sports Injuries, Beijing 100191, China
2. Peking University School of Basic Medical Sciences, Beijing 100191, China
CLC Number:
- R687


| [1] |
Murawski CD, Wolf MR, Araki D, et al. Anatomic anterior cruciate ligament reconstruction: current concepts and future perspective [J]. Cartilage, 2013, 4(3):27S-37S.
doi: 10.1177/1947603513486557 |
| [2] |
Williams RJ, Laurencin CT, Warren RF, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction. Diagnosis and management [J]. Am J Sports Med, 1997, 25(2):261-267.
doi: 10.1177/036354659702500222 |
| [3] |
McAllister DR, Parker RD, Cooper AE, et al. Outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction [J]. Am J Sports Med, 1999, 27(5):562-570.
doi: 10.1177/03635465990270050301 |
| [4] |
Viola R, Marzano N, Vianello R. An unusual epidemic of Staphylococcus-negative infections involving anterior cruciate ligament reconstruction with salvage of the graft and function [J]. Arthroscopy, 2000, 16(2):173-177.
pmid: 10705329 |
| [5] |
Indelli PF, Dillingham M, Fanton G, et al. Septic arthritis in postoperative anterior cruciate ligament reconstruction [J]. Clin Orthop Relat Res, 2002, 398:182-188.
doi: 10.1097/00003086-200205000-00026 |
| [6] |
Schollin-Borg M, Michaёlsson K, Rahme H. Presentation, outcome, and cause of septic arthritis after anterior cruciate ligament reconstruction: a case control study [J]. Arthroscopy, 2003, 19(9):941-947.
pmid: 14608312 |
| [7] |
Burks RT, Friederichs MG, Fink B, et al. Treatment of post-operative anterior cruciate ligament infections with graft removal and early reimplantation [J]. Am J Sports Med, 2003, 31(3):414-418.
doi: 10.1177/03635465030310031501 |
| [8] |
Fong SY, Tan JL. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction [J]. Ann Acad Med Singap, 2004, 33(2):228-234.
pmid: 15098639 |
| [9] |
Musso AD, McCormack RG. Infection after ACL reconstruction: what happens when cultures are negative [J]. Clin J Sport Med, 2005, 15(5):381-384.
pmid: 16162999 |
| [10] |
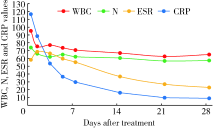
Zalavras CG, Patzakis MJ, Tibone J, et al. Treatment of persistent infection after anterior cruciate ligament surgery [J]. Clin Orthop Relat Res, 2005, 439:52-55.
doi: 10.1097/01.blo.0000181499.49740.e5 |
| [11] |
Judd D, Bottoni C, Kim D, et al. Infections following arthroscopic anterior cruciate ligament reconstruction [J]. Arthroscopy, 2006, 22(4):375-384.
doi: 10.1016/j.arthro.2005.12.002 |
| [12] |
Binnet MS, Basarir K. Risk and outcome of infection after different arthroscopic anterior cruciate ligament reconstruction techniques [J]. Arthroscopy, 2007, 23(8):862-868.
doi: 10.1016/j.arthro.2007.02.008 |
| [13] |
Van Tongel A, Stuyck J, Bellemans J, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: a retrospective analysis of incidence, management and outcome [J]. Am J Sports Med, 2007, 35(7):1059-1063.
doi: 10.1177/0363546507299443 |
| [14] |
Schulz AP, Götze S, Schmidt HG, et al. Septic arthritis of the knee after anterior cruciate ligament surgery: a stage-adapted treatment regimen [J]. Am J Sports Med, 2007, 35(7):1064-1069.
doi: 10.1177/0363546507299744 |
| [15] |
Katz LM, Battaglia TC, Patino P, et al. A retrospective comparison of the incidence of bacterial infection following anterior cruciate ligament reconstruction with autograft versus allograft [J]. Arthroscopy, 2008, 24(12):1330-1335.
doi: 10.1016/j.arthro.2008.07.015 |
| [16] |
Iorio R, Vadalà A, Di VI, et al. Tunnel enlargement after anterior cruciate ligament reconstruction in patients with post-operative septic arthritis [J]. Knee Surg Sports Traumatol Arthrosc, 2008, 16(10):921-927.
doi: 10.1007/s00167-008-0575-1 |
| [17] |
Wang C, Ao Y, Wang J, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: a retrospective analysis of incidence, presentation, treatment, and cause [J]. Arthroscopy, 2009, 25(3):243-249.
doi: 10.1016/j.arthro.2008.10.002 |
| [18] | Sajovic M, NiCAGL , Dernovš EMZ. Septic arthritis of the knee following anterior cruciate ligament reconstruction [J]. Orthop Rev (Pavia), 2009, 1(1):e3. |
| [19] |
Nag HL, Neogi DS, Nataraj AR, et al. Tubercular infection after arthroscopic anterior cruciate ligament reconstruction [J]. Arthroscopy, 2009, 25(2):131-136.
doi: 10.1016/j.arthro.2008.09.009 |
| [20] |
Monaco E, Maestri B, Labianca L, et al. Clinical and radiological outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction [J]. J Orthop Sci, 2010, 15(2):198-203.
doi: 10.1007/s00776-009-1447-3 |
| [21] |
Barker JU, Drakos MC, Maak TG, et al. Effect of graft selection on the incidence of postoperative infection in anterior cruciate ligament reconstruction [J]. Am J Sports Med, 2010, 38(2):281-286.
doi: 10.1177/0363546509346414 |
| [22] |
Benner RW, Shelbourne KD, Freeman H. Infections and patellar tendon ruptures after anterior cruciate ligament reconstruction: a comparison of ipsilateral and contralateral patellar tendon autografts [J]. Am J Sports Med, 2011, 39(3):519-525.
doi: 10.1177/0363546510388163 |
| [23] |
Sonnery-Cottet B, Archbold P, Zayni R, et al. Prevalence of septic arthritis after anterior cruciate ligament reconstruction among professional athletes [J]. Am J Sports Med, 2011, 39(11):2371-2376.
doi: 10.1177/0363546511417567 pmid: 21856928 |
| [24] |
Vertullo CJ, Quick M, Jones A, et al. A surgical technique using presoaked vancomycin hamstring grafts to decrease the risk of infection after anterior cruciate ligament reconstruction [J]. Arthroscopy, 2012, 28(3):337-342.
doi: 10.1016/j.arthro.2011.08.301 |
| [25] |
Schub DL, Schmitz LM, Sakamoto FA, et al. Long-term outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction [J]. Am J Sports Med, 2012, 40(12):2764-2770.
doi: 10.1177/0363546512461903 |
| [26] |
Torres-Claramunt R, Pelfort X, Erquicia J, et al. Knee joint infection after ACL reconstruction: prevalence, management and functional outcomes [J]. Knee Surg Sports Traumatol Arthrosc, 2013, 21(12):2844-2849.
doi: 10.1007/s00167-012-2264-3 |
| [27] |
RisticV , Maljanovic M, Harhaji V, et al. Infections after reconstructions of anterior cruciate ligament [J]. Med Pregl, 2014, 67(1/2):11-15.
doi: 10.2298/MPNS1402011R |
| [28] |
Abdel-Aziz A, Radwan YA, Rizk A. Multiple arthroscopic debridement and graft retention in septic knee arthritis after ACL reconstruction: a prospective case-control study [J]. Int Orthop, 2014, 38(1):73-82.
doi: 10.1007/s00264-013-2123-y pmid: 24100920 |
| [29] |
Boström WH, Mikkelsen C, Forssblad M, et al. Postoperative septic arthritis after anterior cruciate ligament reconstruction: does it affect the outcome? a retrospective controlled study [J]. Arthroscopy, 2014, 30(9):1100-1109.
doi: 10.1016/j.arthro.2014.03.019 |
| [30] |
Calvo R, Figueroa D, Anastasiadis Z, et al. Septic arthritis in ACL reconstruction surgery with hamstring autografts. eleven years of experience [J]. Knee, 2014, 21(3):717-720.
doi: 10.1016/j.knee.2014.01.007 |
| [31] |
Schuster P, Schulz M, Immendoerfer M, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: evaluation of an arthroscopic graft-retaining treatment protocol [J]. Am J Sports Med, 2015, 43(12):3005-3012.
doi: 10.1177/0363546515603054 pmid: 26403209 |
| [32] |
Pérez-Prieto D, Trampuz A, Torres-Claramunt R, et al. Infections after anterior cruciate ligament reconstruction: which antibiotic after arthroscopic debridement? [J]. J Knee Surg, 2017, 30(4):309-313.
doi: 10.1055/s-0036-1584559 pmid: 27367205 |
| [33] |
Hantes ME, Raoulis VA, Doxariotis N, et al. Management of septic arthritis after arthroscopic anterior cruciate ligament reconstruction using a standard surgical protocol [J]. Knee, 2017, 24(3):588-593.
doi: 10.1016/j.knee.2017.02.007 |
| [34] |
Torres-Claramunt R, Gelber P, Pelfort X, et al. Managing septic arthritis after knee ligament reconstruction [J]. Int Orthop, 2016, 40(3):607-614.
doi: 10.1007/s00264-015-2884-6 pmid: 26239533 |
| [35] |
Wang C, Lee YH, Siebold R. Recommendations for the management of septic arthritis after ACL reconstruction [J]. Knee Surg Sports Traumatol Arthrosc, 2014, 22(9):2136-2144.
doi: 10.1007/s00167-013-2648-z |
| [36] |
Muscolo DL, Carbo L, Aponte-Tinao LA, et al. Massive bone loss from fungal infection after anterior cruciate ligament arthroscopic reconstruction [J]. Clin Orthop Relat Res, 2009, 467(9):2420-2425.
doi: 10.1007/s11999-009-0714-0 |
| [37] |
Wang C, Ao Y, Fan X, et al. C-reactive protein and erythrocyte sedimentation rate changes after arthroscopic anterior cruciate ligament reconstruction: guideline to diagnose and monitor postoperative infection [J]. Arthroscopy, 2014, 30(9):1110-1115.
doi: 10.1016/j.arthro.2014.03.025 |
| [38] |
Paci JM, Schweizer SK, Wilbur DM, et al. Results of laboratory evaluation of acute knee effusion after anterior cruciate ligament reconstruction: what is found in patients with a noninfected, painful postoperative knee [J]. Am J Sports Med, 2010, 38(11):2267-2272.
doi: 10.1177/0363546510374573 |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Xueli TIAN, Zhiqiang SONG, Yonghui HUANG, Wei YAO. Analysis of early complications and risk factors in patients with amyotrophic lateral sclerosis after percutaneous endoscopic gastrostomy [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 190-195. |
| [3] | Xiaolin WANG, Shaoyi GUO, Dazhao CHEN, Xijie WEN, Yong HUA, Liang ZHANG, Qin ZHANG. A follow-up study on total hip arthroplasty in patients with systemic lupus erythematosus combined with osteonecrosis of femoral head [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1081-1088. |
| [4] | Fengyi HU, Qingyang MENG, Nayun CHEN, Jianing WANG, Zhenlong LIU, Yong MA, Yuping YANG, Xi GONG, Cheng WANG, Ping LIU, Weili SHI. Clinical efficacy of arthroscopic medial patellofemoral complex reconstruction for recurrent patellar dislocation with high-grade trochlear dysplasia [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 947-955. |
| [5] | Xiaoteng YU, Yixuan HUANG, Xinfei LI, Changfu CHEN, Fangzhou ZHAO, Honggang YING, Zihao TAO, Yiming ZHANG, Liqing XU, Zhihua LI, Kunlin YANG, Liqun ZHOU, Xuesong LI, Zheng ZHAO. Surgical techniques and clinical outcomes of upper urinary tract reconstruction for stone-related ureteral strictures [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 670-675. |
| [6] | Chao ZUO, Guoli WANG, Kunlin YANG, Xinyan CHE, Yisen MENG, Kai ZHANG. Comparison of efficacy and safety of transurethral thulium fiber laser enucleation of prostate in patients with different prostate volumes [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 711-716. |
| [7] | Zhao ZHAO, Weiyu ZHANG, Wenbo YANG, Yongjie ZHANG, Xiaopeng ZHANG, Huiying ZHAO, Gang ZHOU, Qiang WANG. Kidney transplantation in low-age, low-weight children: A report of two cases [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 803-807. |
| [8] | Jianjun SUN, Qianquan MA, Xiaoliang YIN, Chenlong YANG, Jia ZHANG, Suhua CHEN, Chao WU, Jingcheng XIE, Yunfeng HAN, Guozhong LIN, Yu SI, Jun YANG, Haibo WU, Qiang ZHAO. Significance of precise classification of sacral meningeal cysts by multiple dimensions radiographic reconstruction MRI in guiding operative strategy and rehabilitation [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 303-308. |
| [9] | Shiyu QIU, Yang LIAN, Yifan KANG, Lei ZHANG, Yiwang CAI, Xiaofeng SHAN, Zhigang CAI. Personalized mandibular reconstruction assisted by three-dimensional retrieval model based on fully connected neural network and a database of mandibles [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 360-368. |
| [10] | Fei WANG, Xinyue ZHANG, Muqing LIU, Enbo WANG, Denghui DUAN. Clinical application and three-dimensional finite element analysis of along-axis extraction method in mandibular mesial and horizontally impacted third molar surgery [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 106-112. |
| [11] | Jianxun MA, Xi BU, Bi LI. Application of dual chamber round tissue expander in immediate breast reconstruction [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 166-171. |
| [12] | Liwei WANG, Bingchuan LIU, Yinyin QU, Changyi WU, Yun TIAN. Clinical application of multidisciplinary team in the diagnosis and treatment of chronic refractory wounds [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 185-191. |
| [13] | Fangfei XIE, Hong QIAO, Boya LI, Cui YUAN, Fang WANG, Yu SUN, Shuangling LI. Severe malnutrition during pregnancy complicated with acute pyelonephritis causing sepsis, refractory septic shock and multiple organ failure: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 202-207. |
| [14] | Junnan NIE, Jiayun DONG, Ruifang LU. Analysis of soft tissue healing after keratinized tissue augmentation in reconstructed jaws [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 57-64. |
| [15] | Yifan KANG, Yanjun GE, Xiaoming LV, Shang XIE, Xiaofeng SHAN, Zhigang CAI. One-stage mandibular reconstruction combining iliac flap with immediate implant-based denture [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 78-84. |
|
||