Journal of Peking University (Health Sciences) ›› 2022, Vol. 54 ›› Issue (2): 376-380. doi: 10.19723/j.issn.1671-167X.2022.02.028
Previous Articles Next Articles
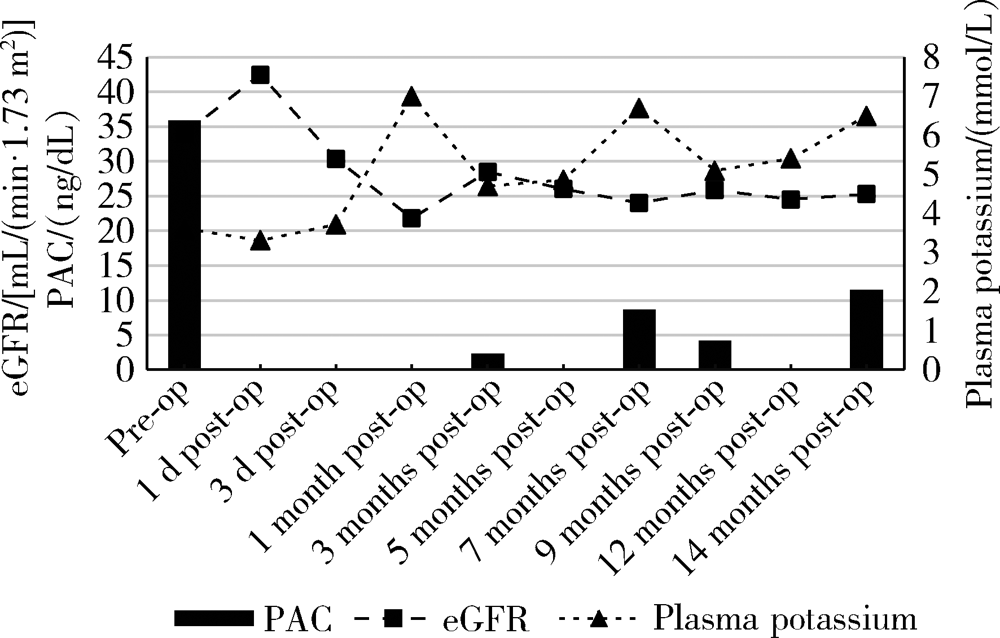
Persistent and serious hyperkalemia after surgery of primary aldosteronism: A case report
WANG Wei1,CAI Lin2,GAO Ying1,GUO Xiao-hui1,ZHANG Jun-qing1,△( )
)
- 1. Department of Endocrinology, Peking University First Hospital, Beijing 100034, China
2. Department of Urology, Peking University First Hospital, Beijing 100034, China
CLC Number:
- R589.4


| [1] |
Huang WT, Chau T, Wu ST, et al. Prolonged hyperkalemia following unilateral adrenalectomy for primary hyperaldosteronism[J]. Clin Nephrol, 2010, 73(5):392-397.
pmid: 20420801 |
| [2] |
Fischer E, Hanslik G, Pallauf A, et al. Prolonged zona glomerulosa insufficiency causing hyperkalemia in primary aldosteronism after adrenalectomy[J]. J Clin Endocrinol Metab, 2012, 97(11):3965-3973.
doi: 10.1210/jc.2012-2234 pmid: 22893716 |
| [3] |
Chiang WF, Cheng CJ, Wu ST, et al. Incidence and factors of post-adrenalectomy hyperkalemia in patients with aldosterone producing adenoma[J]. Clin Chim Acta, 2013, 424(9):114-118.
doi: 10.1016/j.cca.2013.05.017 |
| [4] |
Hibi Y, Hayakawa N, Hasegawa M, et al. Unmasked renal impairment and prolonged hyperkalemia after unilateral adrenalectomy for primary aldosteronism coexisting with primary hyper-parathyroidism: Report of a case[J]. Surg Today, 2015, 45(2):241-246.
doi: 10.1007/s00595-013-0813-0 |
| [5] |
Tahir A, McLaughlin K, Kline G. Severe hyperkalemia following adrenalectomy for aldosteronoma: Prediction, pathogenesis and approach to clinical management: A case series[J]. BMC Endocr Disord, 2016, 16(1):43.
doi: 10.1186/s12902-016-0121-y pmid: 27460219 |
| [6] |
Park KS, Kim JH, Yang YS, et al. Outcomes analysis of surgical and medical treatments for patients with primary aldosteronism[J]. Endocr J, 2017, 64(6):623-632.
doi: 10.1507/endocrj.EJ16-0530 |
| [7] |
Wada N, Shibayama Y, Umakoshi H, et al. Hyperkalemia in both surgically and medically treated patients with primary aldosteronism[J]. J Hum Hypertens, 2017, 31(10):627-632.
doi: 10.1038/jhh.2017.38 pmid: 28540931 |
| [8] |
Takeda M, Yamamoto K, Akasaka H, et al. Clinical characteristics and postoperative outcomes of primary aldosteronism in the elderly[J]. J Clin Endocrinol Metab, 2018, 103(10):3620-3629.
doi: 10.1210/jc.2018-00059 pmid: 30099522 |
| [9] | 丁韶丽, 阎文军, 赫曼, 等. 原发性醛固酮增多症患者肾上腺切除术中并发严重高钾血症1例[J]. 中华麻醉学杂志, 2018, 38(4):509-510. |
| [10] |
Shariq OA, Bancos I, Cronin PA, et al. Contralateral suppression of aldosterone at adrenal venous sampling predicts hyperkalemia following adrenalectomy for primary aldosteronism[J]. Surgery, 2018, 163(1):183-190.
doi: 10.1016/j.surg.2017.07.034 |
| [11] |
Taniguchi R, Koshiyama H, Yamauchi M, et al. A case of aldosterone-producing adenoma with severe postoperative hyperkalemia[J]. Tohoku J Exp Med, 1998, 186(3):215-223.
pmid: 10348217 |
| [1] | Zhaode BU, Mengyu FENG, Ke JI. Practice and reflection on sentinel lymph node navigation surgery for early gastric cancer [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 239-243. |
| [2] | Wen DU, Wenbo ZHANG, Yao YU, Shuo LIU, Huiyu SU, Leihao HU, Zunan TANG, Binzhang WU, Zhen CHEN, Jiaqi LI, Hao WANG, Xin PENG. Exploration and clinical application of the "digital and intelligent surgery" diagnosis and treatment workflow for oral and maxillofacial tumors [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 278-284. |
| [3] | Jingheng WU, Yunhao XUE, Shanlin CHEN, Yintao GUO, Yuntao LIU, Wei ZHANG. Super microsurgical lymphaticovenular anastomosis for limb lymphedema: An outcome analysis based on clinical stage and indocyanine green pattern [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 359-364. |
| [4] | Lu YU, Ling WU, Xiaojing LIU, Zili LI. Feasibility study of a surgical planning protocol for orthognathic surgery utilizing similarity retrieval from database: A randomized controlled trial [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 145-152. |
| [5] | Rentao TANG, Liuchang YANG, Jie NIE, Xiaoyan WANG. Microbial communities in extraradicular infections of post-treatment apical periodontitis without or with sinus tracts [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 43-49. |
| [6] | Zhemin LI, Jiafu JI, Guoxin LI, Ziyu LI, Zhaode BU, Xiangyu GAO, Di DONG, Lei TANG, Xiaofang XING, Shuqin JIA, Ting GUO, Lianhai ZHANG, Fei SHAN, Xin JI, Anqiang WANG. Development and dissemination of precision medicine approaches in gastric cancer management [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 864-867. |
| [7] | Bowen LI, Qiang ZHANG, Yixin SUN. Establishment and validation of a risk prediction model for scoliosis after Nuss procedure in children and young adults with pectus excavatum [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 941-946. |
| [8] | Xiaoteng YU, Yixuan HUANG, Xinfei LI, Changfu CHEN, Fangzhou ZHAO, Honggang YING, Zihao TAO, Yiming ZHANG, Liqing XU, Zhihua LI, Kunlin YANG, Liqun ZHOU, Xuesong LI, Zheng ZHAO. Surgical techniques and clinical outcomes of upper urinary tract reconstruction for stone-related ureteral strictures [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 670-675. |
| [9] | Wanwei HUANG, Xianshen SHA, Yibao ZHANG, Guohao WU, Feng LUO, Zhihui CHEN, Dongming YE, Xuesong LI, Caiyong LAI. Total 3D laparoscopic ileal ureters replacement for bilateral ureters combined with bladder augmentation in the management of post-radiotherapy bilateral ureteral strictures and contracted bladder [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 789-795. |
| [10] | Lianlian CHEN, Zhangying CAI, Linna YE, Jie LI. Current status and influencing factors of kinesiophobia in patients with lumbar disc herniation after lumbar fusion surgery [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 317-322. |
| [11] | Lei YU, Wenbo YANG, Yufan YANG, Qiang WANG. Renal autotransplantation for the treatment of complex renal aneurysm in a child: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 396-399. |
| [12] | Yang TIAN, Yongzheng HAN, Jiao LI, Mingya WANG, Yinyin QU, Jingchao FANG, Hui JIN, Min LI, Jun WANG, Mao XU, Shenglin WANG, Xiangyang GUO. Incidence and risk factors of postoperative epidural hematoma following anterior cervical spine surgery [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1058-1064. |
| [13] | Le YU,Shaohui DENG,Fan ZHANG,Ye YAN,Jianfei YE,Shudong ZHANG. Clinicopathological characteristics and prognosis of multilocular cystic renal neoplasm of low malignant potential [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 661-666. |
| [14] | Kewei CHEN,Shaohui DENG,Zhuo LIU,Hongxian ZHANG,Lulin MA,Shudong ZHANG. Discussion on the surgical timing of rupture and hemorrhage of renal angiomyolipoma [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 326-331. |
| [15] | Silan AN,Qunyi ZHENG,Kai WANG,Shan GAO. Characteristics and influencing factors of early pain in patients after total knee arthroplasty [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 167-173. |
|
||