Journal of Peking University (Health Sciences) ›› 2022, Vol. 54 ›› Issue (2): 381-385. doi: 10.19723/j.issn.1671-167X.2022.02.029
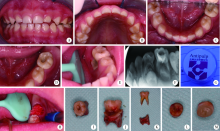
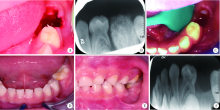
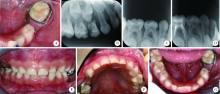
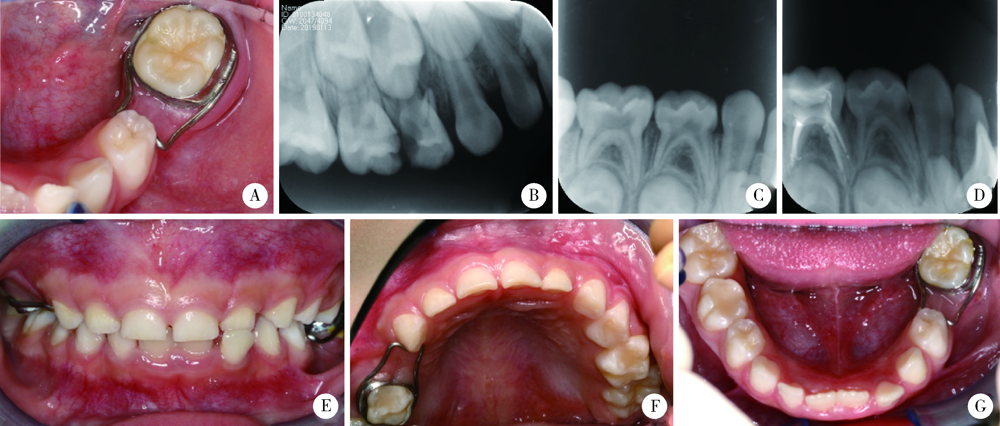
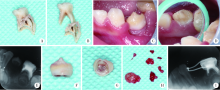
Early loss of primary molar and permanent tooth germ caused by the use of devitalizer during primary molar root canal therapy: Two cases report
TIAN Jing,QIN Man,CHEN Jie,XIA Bin( )
)
- Department of Pediatric Dentistry, Peking University School and Hospital of Stomatology & National Center of Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomatology & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
CLC Number:
- R788



| [1] | 高学军, 岳林. 牙体牙髓病学[M]. 2版. 北京: 北京大学医学出版社, 2013: 478. |
| [2] | 葛立宏. 儿童口腔医学[M]. 4版. 北京: 人民卫生出版社, 2012. |
| [3] | 葛立宏. 儿童口腔医学[M]. 2版. 北京: 北京大学医学出版社, 2013: 295. |
| [4] | 夏斌, 秦满, 葛立宏. 我国儿童口腔科医师临床诊疗工作调查分析[J]. 现代口腔医学杂志, 2007, 21(1):80-82. |
| [5] | 包晶, 汪奕, 姜德龙, 等. Antipulp对儿童乳磨牙牙髓失活的临床疗效观察[J]. 吉林医学, 2014, 35(25):5644-5645. |
| [6] | 鲁伟, 高玉萍, 冯琼芬, 等. 三氧化二砷泄漏致牙周组织及牙槽骨坏死20例[J]. 中华口腔医学杂志, 2011, 46(9):575-576. |
| [7] | 沈国华, 翟启善. 碘中和法治疗砷性根尖周炎70例临床报告: 全国第四次牙体牙髓病学术会议[C]. 上海: [出版者不详], 1995. |
| [8] | 张敬雷, 窦金红. 氮酮多聚甲醛致牙龈严重烧伤[J]. 临床误诊误治, 2004, 17(2):143. |
| [1] | Xinying WANG, Xueyuan CHENG, Mengjun ZHANG, Fei LI, Jinyu DUAN, Jing QIAO. Effect of concentrated growth factors in guided tissue regeneration for the treatment of mandibular molar furcation lesions [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 372-379. |
| [2] | Yue WANG, Yuhong LIANG. Florid cemento-osseous dysplasia: A case report [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 220-224. |
| [3] | Lijuan MA, Yonghui TENG, Yong WANG, Yijiao ZHAO, Xinyue ZHANG, Qingzhao QIN, Dong YIN. Three-dimensional finite element analysis of digital wire loop space maintainers for missing deciduous teeth [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 376-383. |
| [4] | Fei WANG, Xinyue ZHANG, Muqing LIU, Enbo WANG, Denghui DUAN. Clinical application and three-dimensional finite element analysis of along-axis extraction method in mandibular mesial and horizontally impacted third molar surgery [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 106-112. |
| [5] | Yutong SHI, Yiping WEI, Wenjie HU, Tao XU, Haoyun ZHANG. Evaluation of micro crestal flap-alveolar ridge preservation following extraction of mandibular molars with severe periodontitis [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 33-41. |
| [6] | Chen CHEN,Yuhong LIANG. Root canal therapy of maxillary molars with atypical canals: A report of three cases [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 190-195. |
| [7] | FENG Sha-wei,GUO Hui,WANG Yong,ZHAO Yi-jiao,LIU He. Initial establishment of digital reference standardized crown models of the primary teeth [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 327-334. |
| [8] | CHEN Zhen,GU Bao-xin,TANG Yu-fang,YAN Zi-yu,NI Fang-duan,CUI Nian-hui. Constructions of the scale of difficulty in the extraction of impacted mandibular third molars by using Delphi method [J]. Journal of Peking University (Health Sciences), 2022, 54(1): 100-104. |
| [9] | JIANG You-sheng,FENG Lin,GAO Xue-jun. Influence of base materials on stress distribution in endodontically treated maxillary premolars restored with endocrowns [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 764-769. |
| [10] | Wei QI,Jian-nan LI,Jing-ren ZHAO,Hai-xia XING,Jie PAN. Effect of triangular flap design and healing procedure on the sequelae after extraction of impacted lower third molars [J]. Journal of Peking University(Health Sciences), 2019, 51(5): 949-953. |
| [11] | Li-ping ZHAO,Wen-jie HU,Tao XU,Ya-lin ZHAN,Yi-ping WEI,Min ZHEN,Cui WANG. Two procedures for ridge preservation of molar extraction sites affected by severe bone defect due to advanced periodontitis [J]. Journal of Peking University(Health Sciences), 2019, 51(3): 579-585. |
| [12] | Qiong ZHOU,Chu-fang PENG,Man QIN. Near-infrared light transillumination for detection of incipient proximal caries in primary molars [J]. Journal of Peking University(Health Sciences), 2019, 51(1): 59-64. |
| [13] | Yue LEI,Ying-ting YANG,Yuan ZHAN. Evaluation of bioceramic putty repairment in primary molars pulpotomy [J]. Journal of Peking University(Health Sciences), 2019, 51(1): 70-74. |
| [14] | WU Ling, LIU Xiao-jing, LI Zi-li, WANG Xing. Evaluation of accuracy of virtual occlusal definition in Angle class Ⅰ molar relationship [J]. Journal of Peking University(Health Sciences), 2018, 50(1): 154-159. |
| [15] | ZHANG Ming-ming, ZHENG Ying-dong, LIANG Yu-hong. A prognostic model for assessment of outcome of root canal treatment in teeth with pulpitis or apical periodontitis#br# [J]. Journal of Peking University(Health Sciences), 2018, 50(1): 123-130. |
|
||