Journal of Peking University (Health Sciences) ›› 2024, Vol. 56 ›› Issue (4): 631-635. doi: 10.19723/j.issn.1671-167X.2024.04.014
Previous Articles Next Articles
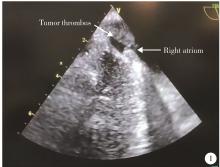
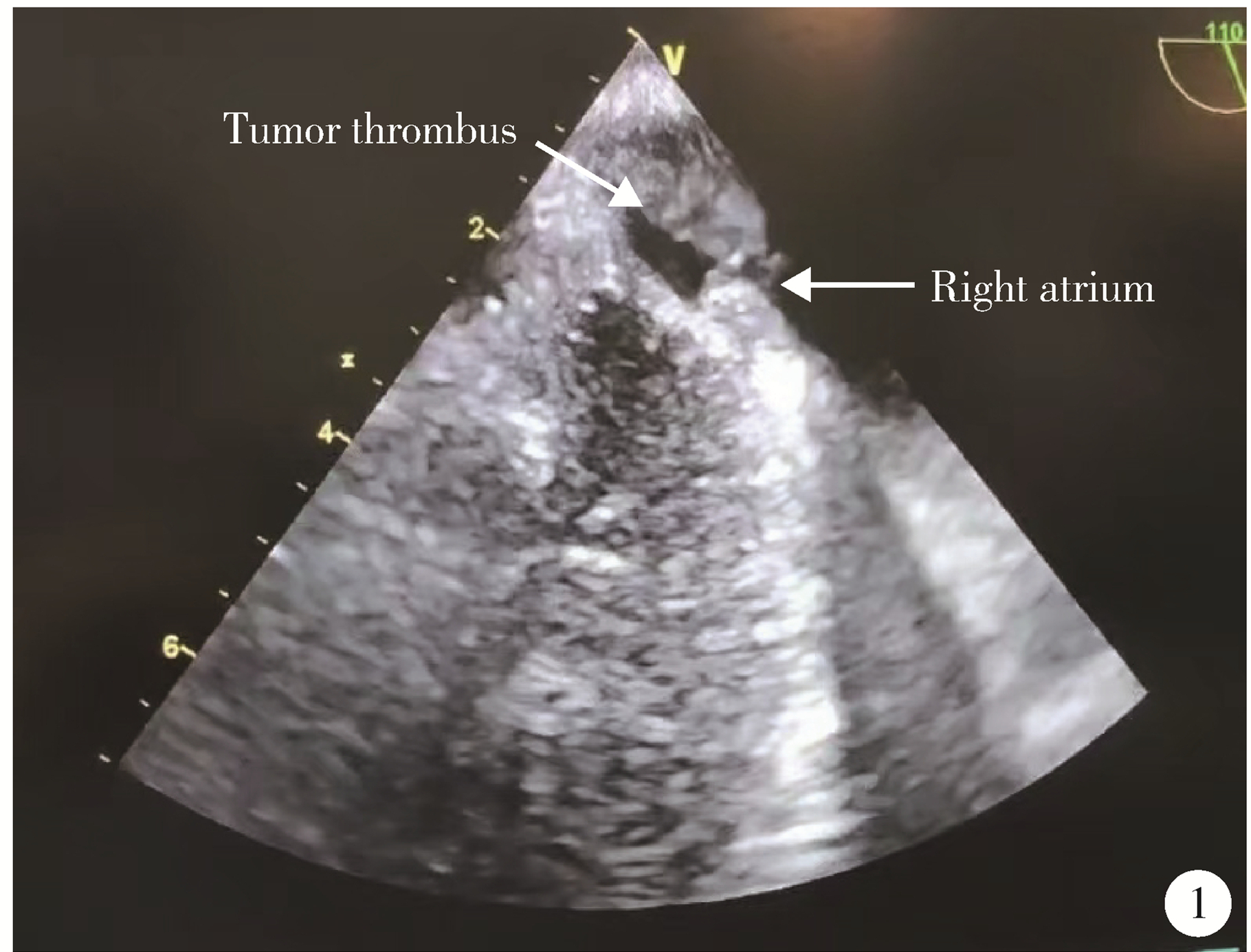
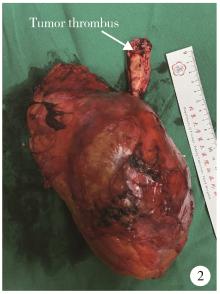
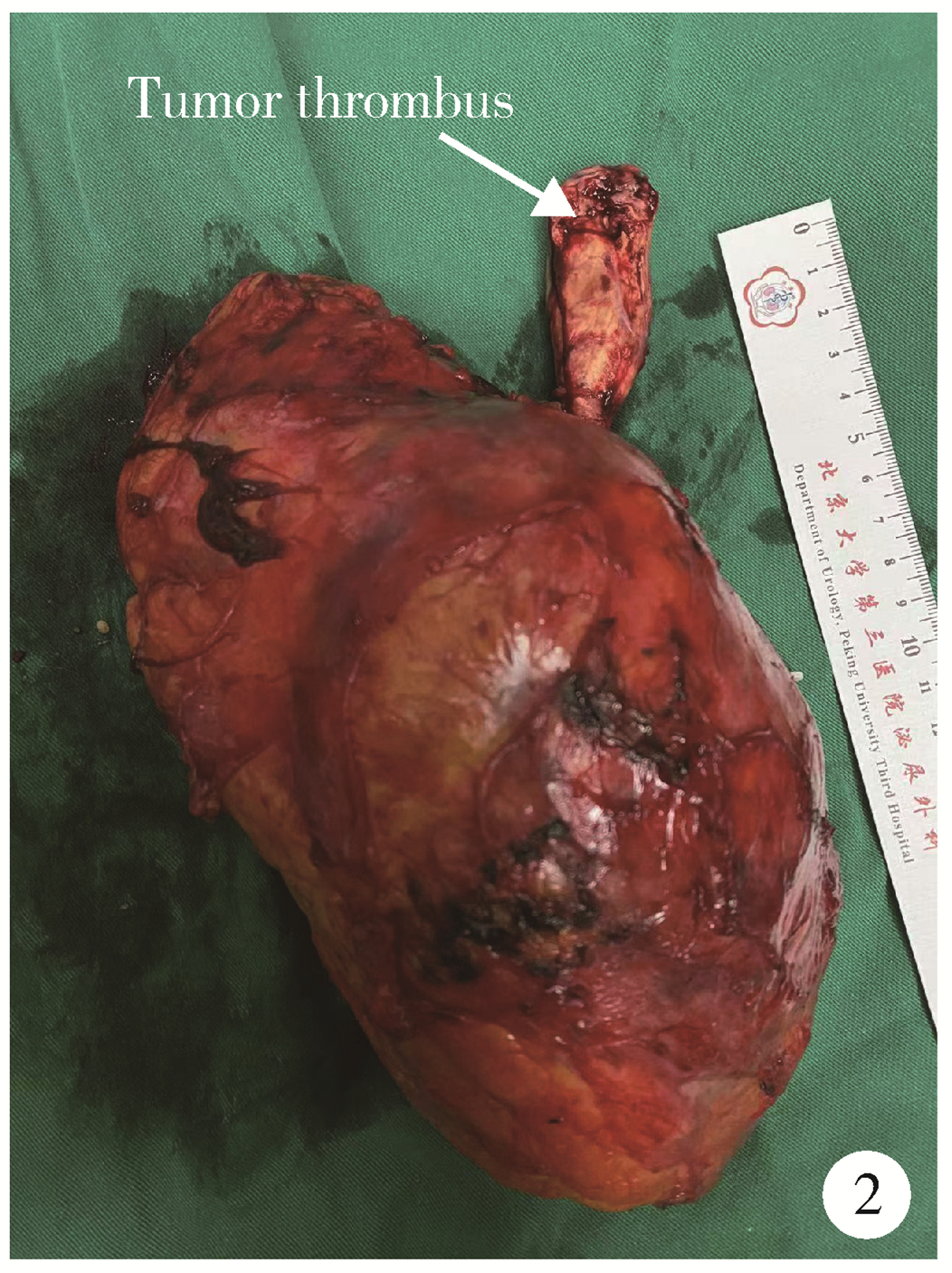
Clinical effects of transesophageal echocardiography in different surgical methods for nephrectomy combined with Mayo Ⅲ-Ⅳ vena tumor thrombectomy
Jie YANG1,Jieli FENG1,*( ),Shudong ZHANG2,Lulin MA2,Qing ZHENG3
),Shudong ZHANG2,Lulin MA2,Qing ZHENG3
- 1. Department of Cardiology, Peking University Third Hospital, Beijing 100191, China
2. Department of Urology, Peking University Third Hospital, Beijing 100191, China
3. Department of Anesthesiology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R737.11
| 1 |
中华医学会泌尿外科学分会中国肾癌联盟, 中国肾癌伴下腔静脉癌栓诊疗协作组. 肾癌伴静脉癌栓诊治专家共识[J]. 中华泌尿外科杂志, 2018, 39 (12): 881- 884.
doi: 10.3760/cma.j.issn.1000-6702.2018.12.001 |
| 2 | 马潞林, 邱敏, 田晓军, 等. 改良泌尿系统肿瘤伴静脉癌栓的诊断与治疗[M]. 北京: 北京大学医学出版社, 2024: 75- 81. |
| 3 |
赵勋, 刘茁, 马潞林. 肾癌合并Mayo Ⅳ级下腔静脉癌栓的诊治进展[J]. 中华泌尿外科杂志, 2019, 40 (6): 471- 473.
doi: 10.3760/cma.j.issn.1000-6702.2019.06.021 |
| 4 | 王迎春, 孔延亮, 刘钰苇, 等. 术前CTA评估大体积肾癌肾动静脉解剖及癌栓[J]. 中国介入影像与治疗学, 2020, 17 (9): 561- 564. |
| 5 | 马鑫, 何志嵩, 马潞林, 等. 机器人肾癌伴静脉癌栓切除术专家共识[J]. 微创泌尿外科杂志, 2023, 12 (1): 1- 7. |
| 6 |
Jurado A , Romeo A , Gueglio G , et al. Current trends in management of renal cell carcinoma with venous thrombus extension[J]. Curr Urol Rep, 2021, 22 (4): 23- 31.
doi: 10.1007/s11934-021-01036-y |
| 7 |
Yuan SM . Surgical treatment of renal cell carcinoma with inferior vena cava tumor thrombus[J]. Surg Today, 2022, 52 (8): 1125- 1133.
doi: 10.1007/s00595-021-02429-9 |
| 8 | 严旭芝, 王硕, 刘秋礼, 等. 根治性肾切除联合下腔静脉癌栓取出机器人辅助与开放手术的临床疗效对比[J]. 陆军军医大学学报, 2023, 45 (20): 2099- 2105. |
| 9 |
彭程, 黄庆波, 陈勇辉, 等. 肾癌伴Mayo Ⅳ级下腔静脉瘤栓不同术式疗效的多中心回顾性研究[J]. 中华泌尿外科杂志, 2022, 43 (5): 324- 329.
doi: 10.3760/cma.j.cn112330-20220317-00121 |
| 10 |
Bissada NK , Yakout HH , Babanouri A , et al. Longterm expe-rience with management of renal cell carcinoma involving the inferior vena cava[J]. Urology, 2003, 61 (1): 89- 92.
doi: 10.1016/S0090-4295(02)02119-2 |
| 11 | 李丽伟, 刘茁驰, 王国良, 等. 肾癌伴下腔静脉瘤栓合并血栓的多种影像学比较[J]. 北京大学学报(医学版), 2019, 51 (4): 678- 683. |
| 12 | 贾江华, 李旭泽, 王凤, 等. 经食道超声心动图在肾癌伴下腔静脉癌栓手术治疗中的应用[J]. 中国医学科学院学报, 2023, 45 (1): 28- 32. |
| 13 |
Meersch M , Schmidt C , Zarbock A . Echophysiology: The transesophageal echo probe as a noninvasive Swan-Ganz catheter[J]. Curr Opin Anaesthesiol, 2016, 29 (1): 36- 45.
doi: 10.1097/ACO.0000000000000277 |
| 14 |
Hahn RT , Abraham T , Adams MS , et al. Guidelines for perfor-ming a comprehensive transesophageal echocardiographic examination: Recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists[J]. J Am Soc Echocardiogr, 2013, 26 (9): 921- 964.
doi: 10.1016/j.echo.2013.07.009 |
| [1] | Qiming ZHANG, Zebo CHEN, Yu TIAN, Dameng PAN, Lei LIU, Hongxian ZHANG, Lei ZHAO, Shudong ZHANG, Lulin MA, Xiaofei HOU. Experience summary of robot-assisted laparoscopic transplant nephrectomy [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 666-669. |
| [2] | Zezhen ZHOU, Liyuan GE, Fan ZHANG, Shaohui DENG, Ye YAN, Hongxian ZHANG, Guoliang WANG, Lei LIU, Yi HUANG, Shudong ZHANG. A retrospective matching study of partial nephrectomy and radical nephrectomy for pathological T3a stage renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 704-710. |
| [3] | Fan SHU,Yichang HAO,Zhanyi ZHANG,Shaohui DENG,Hongxian ZHANG,Lei LIU,Guoliang WANG,Xiaojun TIAN,Lei ZHAO,Lulin MA,Shudong ZHANG. Functional and oncologic outcomes of partial nephrectomy for cystic renal cell carcinoma: A single-center retrospective study [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 667-672. |
| [4] | Kewei CHEN,Zhuo LIU,Shaohui DENG,Fan ZHANG,Jianfei YE,Guoliang WANG,Shudong ZHANG. Clinical diagnosis and treatment of renal angiomyolipoma with inferior vena cava tumor thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 617-623. |
| [5] | Min QIU,You-long ZONG,Bin-shuai WANG,Bin YANG,Chu-xiao XU,Zheng-hui SUN,Min LU,Lei ZHAO,Jian LU,Cheng LIU,Xiao-jun TIAN,Lu-lin MA. Treatment outcome of laparoscopic partial nephrectomy in patients with renal tumors of moderate to high complexity [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 833-837. |
| [6] | Quan ZHANG,Hai-feng SONG,Bing-lei MA,Zhe-nan ZHANG,Chao-hui ZHOU,Ao-lin LI,Jun LIU,Lei LIANG,Shi-yu ZHU,Qian ZHANG. Pre-operative prognostic nutritional index as a predictive factor for prognosis in non-metastatic renal cell carcinoma treated with surgery [J]. Journal of Peking University (Health Sciences), 2023, 55(1): 149-155. |
| [7] | QIU Min,WANG Lu,DENG Shao-hui,TA Peng-fei,GUO Wei,LU Jian,LIU Cheng,MA Lu-lin. Primary application of Gerota’s fascia suspension device in retroperitoneal laparoscopic partial nephrectomy [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 789-792. |
| [8] | HAN Song-chen,HUANG Zi-xiong,LIU Hui-xin,XU Tao. Renal functional compensation after unilateral radical nephrectomy of renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 680-685. |
| [9] | LI Xin-fei, PENG Yi-ji, YU Xiao-teng, XIONG Sheng-wei, CHENG Si-da, DING Guang-pu, YANG Kun-lin, TANG Qi, MI Yue, WU Jing-yun, ZHANG Peng, XIE Jia-xin, HAO Han, WANG He, QIU Jian-xing, YANG Jian, LI Xue-song, ZHOU Li-qun. Three dimensional nephrometry system for partial nephrectomy: Our initial exploration [J]. Journal of Peking University (Health Sciences), 2021, 53(3): 613-622. |
| [10] | Shu-dong ZHANG,Peng HONG,Bin-shuai WANG,Shao-hui DENG,Fan ZHANG,Li-yuan TAO,Cai-guang CAO,Zhen-hua HU,Lu-lin MA. Usefulness of the indocyanine green fluorescence imaging technique in laparoscopic partial nephrectomy [J]. Journal of Peking University (Health Sciences), 2020, 52(4): 657-662. |
| [11] | ZHAO Lei, MA Lu-lin, ZHANG Hong-xian, HOU Xiao-fei, LIU Lei, FU Yan, KOU Yun-geng, SONG Yi-meng. Technical improvement in retroperitoneal laparoscopic living donor nephrectomy: report of 193 cases [J]. Journal of Peking University(Health Sciences), 2017, 49(5): 867-871. |
| [12] | LIANG Yin-hua, ZU Xiong-bing, CHENG Xu, LIU Long-fei. Retroperitoneal laparoscopic with renal pedicle rotation for partial nephrectomy of ventro-renal tumor [J]. Journal of Peking University(Health Sciences), 2017, 49(4): 608-612. |
| [13] | PENG Ding*, LI Xue-song*, ZHANG Cui-jian, YANG Kai-wei, TANG Qi, ZHANG Lei, YU Xiao-teng, HE Zhi-song, ZHOU Li-qun. Prognostic factors of patients with T3N0M0 renal cell carcinoma: a single-center retrospective study of 182 patients [J]. Journal of Peking University(Health Sciences), 2016, 48(5): 806-811. |
| [14] | QIU Min, LU Jian, MA Lu-Lin, YAN Ye, ZHANG Shu-Dong. Retroperitoneal laparoscopic partial nephrectomy for treatment of cystic nephroma:one case report [J]. Journal of Peking University(Health Sciences), 2014, 46(4): 650-652. |
| [15] | ZHANG Shu-Dong, MA Lu-Lin, HUANG Yi, ZHANG Hong-Xian, LIU Ke, QIU Min. Transabdominal laparoscopic radical nephrectomy of modified Pfannenstiel incision [J]. Journal of Peking University(Health Sciences), 2014, 46(4): 638-641. |
|
||