Journal of Peking University (Health Sciences) ›› 2024, Vol. 56 ›› Issue (4): 624-630. doi: 10.19723/j.issn.1671-167X.2024.04.013
Previous Articles Next Articles
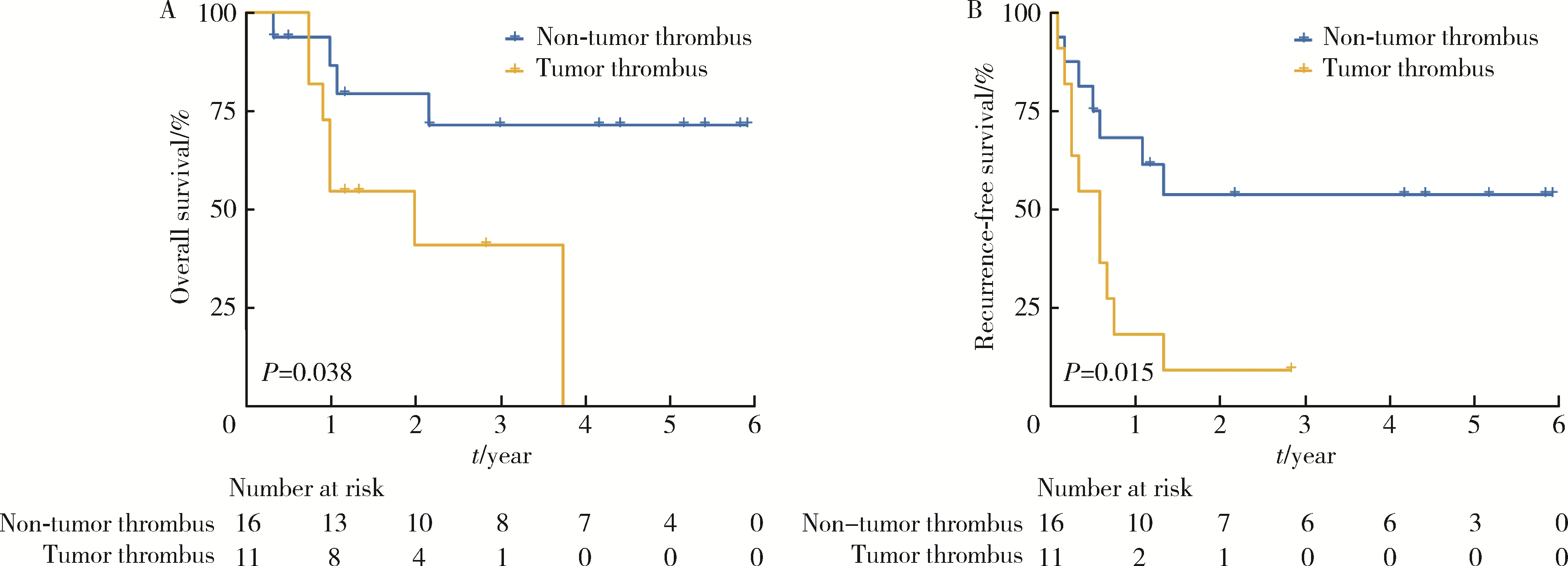
Clinical treatment and prognosis of adrenocortical carcinoma with venous tumor thrombus
Shuai LIU,Lei LIU,Zhuo LIU,Fan ZHANG,Lulin MA,Xiaojun TIAN,Xiaofei HOU,Guoliang WANG,Lei ZHAO,Shudong ZHANG*( )
)
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R699.3

| 1 |
Calissendorff J , Calissendorff F , Falhammar H . Adrenocortical cancer: Mortality, hormone secretion, proliferation and urine ste-roids: Experience from a single centre spanning three decades[J]. BMC Endocr Disord, 2016, 16, 15.
doi: 10.1186/s12902-016-0095-9 |
| 2 |
De Filpo G , Mannelli M , Canu L . Adrenocortical carcinoma: Current treatment options[J]. Curr Opin Oncol, 2021, 33 (1): 16- 22.
doi: 10.1097/CCO.0000000000000695 |
| 3 |
Brönimann S , Garstka N , Remzi M . Treatment of adrenocortical carcinoma: Oncological and endocrine outcomes[J]. Curr Opin Urol, 2023, 33 (1): 50- 58.
doi: 10.1097/MOU.0000000000001045 |
| 4 |
Xu WH , Wu J , Wang J , et al. Screening and identification of potential prognostic biomarkers in adrenocortical carcinoma[J]. Front Genet, 2019, 10, 821.
doi: 10.3389/fgene.2019.00821 |
| 5 | 邓建华, 李汉忠, 纪志刚, 等. 肾上腺皮质癌的综合治疗[J]. 北京大学学报(医学版), 2019, 51 (2): 298- 301. |
| 6 |
Quinones-Baldrich W , Alktaifi A , Eilber F , et al. Inferior vena cava resection and reconstruction for retroperitoneal tumor excision[J]. J Vasc Surg, 2012, 55 (5): 1386- 1393.
doi: 10.1016/j.jvs.2011.11.054 |
| 7 |
Schwarzbach MH , Hormann Y , Hinz U , et al. Clinical results of surgery for retroperitoneal sarcoma with major blood vessel involvement[J]. J Vasc Surg, 2006, 44 (1): 46- 55.
doi: 10.1016/j.jvs.2006.03.001 |
| 8 |
Nooromid MJ , Ju MH , Havelka GE , et al. Fifteen-year expe-rience with renal cell carcinoma with associated venous tumor thrombus[J]. Surgery, 2016, 160 (4): 915- 923.
doi: 10.1016/j.surg.2016.06.029 |
| 9 |
Shao P , Li J , Qin C , et al. Laparoscopic radical nephrectomy and inferior vena cava thrombectomy in the treatment of renal cell carcinoma[J]. Eur Urol, 2015, 68 (1): 115- 122.
doi: 10.1016/j.eururo.2014.12.011 |
| 10 |
Agochukwu N , Shuch B . Clinical management of renal cell carcinoma with venous tumor thrombus[J]. World J Urol, 2014, 32 (3): 581- 589.
doi: 10.1007/s00345-014-1276-7 |
| 11 |
Fairweather M , Raut CP . Nephrectomy for retroperitoneal sarcoma: Stay calm and (cautiously) carry on[J]. Ann Surg Oncol, 2021, 28 (3): 1275- 1277.
doi: 10.1245/s10434-020-09293-w |
| 12 |
Liu Z , Ge L , Liu L , et al. Clinical experience and management strategy of retroperitoneal tumor with venous tumor thrombus involvement[J]. Front Oncol, 2022, 12, 873729.
doi: 10.3389/fonc.2022.873729 |
| 13 | Jannello LMI, Incesu RB, Morra S, et al. The European Network for the Study of Adrenal Tumors staging system (2015): A United States validation[J/OL]. J Clin Endocrinol Metab, 2024: dgae047[2024-02-18]. doi: 10.1210/clinem/dgae047. |
| 14 |
Liu Z , Zhao X , Ge L , et al. Completely laparoscopic versus open radical nephrectomy and infrahepatic tumor thrombectomy: Comparison of surgical complexity and prognosis[J]. Asian J Surg, 2021, 44 (4): 641- 648.
doi: 10.1016/j.asjsur.2020.12.003 |
| 15 |
Zhang G , Li X , Sun G , et al. Clinical analysis of Kimura's di-sease in 24 cases from China[J]. BMC Surg, 2020, 20 (1): 1.
doi: 10.1186/s12893-019-0673-7 |
| 16 |
Liu Z , Li Y , Zhang Y , et al. PUTH grading system for urinary tumor with supradiaphragmatic tumor thrombus: Different surgical techniques for different tumor characteristics[J]. Front Oncol, 2022, 11, 735145.
doi: 10.3389/fonc.2021.735145 |
| 17 |
Blute ML , Leibovich BC , Lohse CM , et al. The Mayo clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus[J]. BJU Int, 2004, 94 (1): 33- 41.
doi: 10.1111/j.1464-410X.2004.04897.x |
| 18 |
Laan DV , Thiels CA , Glasgow A , et al. Adrenocortical carcinoma with inferior vena cava tumor thrombus[J]. Surgery, 2017, 161 (1): 240- 248.
doi: 10.1016/j.surg.2016.07.040 |
| 19 |
Piardi T , Lhuaire M , Memeo R , et al. Laparoscopic Pringle maneuver: How we do it?[J]. Hepatobiliary Surg Nutr, 2016, 5 (4): 345- 349.
doi: 10.21037/hbsn.2015.11.01 |
| 20 |
Fiore M , Colombo C , Locati P , et al. Surgical technique, morbi-dity, and outcome of primary retroperitoneal sarcoma involving inferior vena cava[J]. Ann Surg Oncol, 2012, 19 (2): 511- 518.
doi: 10.1245/s10434-011-1954-2 |
| 21 | 刘磊, 王国良, 马潞林, 等. 肾上腺区巨大肿瘤合并瘤栓的诊断与治疗[J]. 北京大学学报(医学版), 2019, 51 (4): 684- 688. |
| 22 |
杨华安, 郭胜杰. 肾上腺皮质癌合并静脉癌栓的手术治疗及预后[J]. 实用医学杂志, 2020, 36 (10): 1344- 1348.
doi: 10.3969/j.issn.1006-5725.2020.10.015 |
| 23 |
Zhao X , Liu Z , Zhang H , et al. PKUTHLP score: A comprehensive system to predict surgical approach in radical nephrectomy and thrombectomy[J]. Oncol Lett, 2020, 20 (1): 201- 208.
doi: 10.3892/ol.2020.11571 |
| 24 | Vuong NS , Ferriere JM , Michiels C , et al. Robot-assisted versus open surgery for radical nephrectomy with level 1-2 vena cava tumor thrombectomy: A French monocenter experience (UroCCR study #73)[J]. Minerva Urol Nephrol, 2021, 73 (4): 498- 508. |
| 25 |
Treiger BF , Humphrey LS , Peterson CV , et al. Transesophageal echocardiography in renal cell carcinoma: An accurate diagnostic technique for intracaval neoplastic extension[J]. J Urol, 1991, 145 (6): 1138- 1140.
doi: 10.1016/S0022-5347(17)38556-7 |
| [1] | Bo PENG, Fangfang LIU, Wei YANG, Ruiping XU, Lei CHEN, Baozhong LI, Xinjia WANG, Ji KE, Wenlei YANG, Yu HE, Zhen LIU, Bolin HOU, Liqun ZHANG, Miaoping LIN, Lixin ZHANG, Fan ZHANG, Fen CAI, Huawen XU, Mengfei LIU, Ying LIU, Yaqi PAN, Zhonghu HE, Yang KE. Perioperative hyperglycemia predicts poorer prognosis of esophageal squamous cell carcinoma patients treated with esophagectomy [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 567-574. |
| [2] | Fan SHU, Liyuan GE, Hanzhang DENG, Haoming YIN, Junyong OU, Shaohui DENG, Yichang HAO, Min LU, Zhanyi ZHANG, Peichen DUAN, Shudong ZHANG. Molecular characteristics for poor prognosis related renal cell carcinoma with lymph metastases [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 631-640. |
| [3] | Lingfu ZHANG, Ming CHEN, Xiaoyu ZHAO, Gang WANG, Long CUI, Xiaofeng LING, Lixin WANG, Zhi XU, Limei GUO, Chunsheng HOU. Gross classification of gallbladder cancer with primary lesion limited to the gallbladder wall and its correlation with prognosis and precancerous lesions [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 184-189. |
| [4] | Boda GUO, Min LU, Guoliang WANG, Hongxian ZHANG, Lei LIU, Xiaofei HOU, Lei ZHAO, Xiaojun TIAN, Shudong ZHANG. Clinicopathological and prognostic differences between clear cell and non-clear cell renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 644-649. |
| [5] | Zhanyi ZHANG, Min LU, Yuehao SUN, Jinghan DONG, Xiaofei HOU, Chunlei XIAO, Guoliang WANG, Xiaojun TIAN, Lulin MA, Hongxian ZHANG, Shudong ZHANG. Clinicopathological features and survival analysis of TFE3-rearranged renal cell carcinoma with venous tumor thrombus [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 650-661. |
| [6] | Shuai LIU, Zhuo LIU, Yunhe GUAN, Guoliang WANG, Xiaojun TIAN, Hongxian ZHANG, Lei LIU, Lulin MA, Shudong ZHANG. Robot-assisted laparoscopic inferior vena cava segmental resection for renal tumor with tumor thrombus invading the vascular wall [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 796-802. |
| [7] | Weihao LI, Jing LI, Xuemin ZHANG, Wei LI, Qingle LI, Xiaoming ZHANG. Effect of intraoperative blood salvage autotransfusion on the prognosis of patients after carotid body tumor resection [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 272-276. |
| [8] | Yaqing MAO, Zhen CHEN, Yao YU, Wenbo ZHANG, Yang LIU, Xin PENG. Impact of type 2 diabetes mellitus on the prognosis of patients with oral squamous cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(6): 1089-1096. |
| [9] | Junyong OU,Kunming NI,Lulin MA,Guoliang WANG,Ye YAN,Bin YANG,Gengwu LI,Haodong SONG,Min LU,Jianfei YE,Shudong ZHANG. Prognostic factors of patients with muscle invasive bladder cancer with intermediate-to-high risk prostate cancer [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 582-588. |
| [10] | Kewei CHEN,Zhuo LIU,Shaohui DENG,Fan ZHANG,Jianfei YE,Guoliang WANG,Shudong ZHANG. Clinical diagnosis and treatment of renal angiomyolipoma with inferior vena cava tumor thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 617-623. |
| [11] | Jie YANG,Jieli FENG,Shudong ZHANG,Lulin MA,Qing ZHENG. Clinical effects of transesophageal echocardiography in different surgical methods for nephrectomy combined with Mayo Ⅲ-Ⅳ vena tumor thrombectomy [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 631-635. |
| [12] | Binshuai WANG,Min QIU,Qianjin ZHANG,Maofeng TIAN,Lei LIU,Guoliang WANG,Min LU,Xiaojun TIAN,Shudong ZHANG. Experience in diagnosis and treatment of 6 cases of renal Ewing's sarcoma with venous thrombus [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 636-639. |
| [13] | Le YU,Shaohui DENG,Fan ZHANG,Ye YAN,Jianfei YE,Shudong ZHANG. Clinicopathological characteristics and prognosis of multilocular cystic renal neoplasm of low malignant potential [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 661-666. |
| [14] | Zezhen ZHOU,Shaohui DENG,Ye YAN,Fan ZHANG,Yichang HAO,Liyuan GE,Hongxian ZHANG,Guoliang WANG,Shudong ZHANG. Predicting the 3-year tumor-specific survival in patients with T3a non-metastatic renal cell carcinoma [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 673-679. |
| [15] | Yangyi FANG,Qiang LI,Zhigao HUANG,Min LU,Kai HONG,Shudong ZHANG. Well-differentiated papillary mesothelial tumour of the tunica vaginalis: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 741-744. |
|
||